On the evening of the twenty-fourth of March, 1882, in a cramped lecture room in Berlin, a provincial medical officer held up to view the cause of the disease that was then killing one European in seven. It was a rod so slender, and so unwilling to take up any dye, that no one had ever seen it; to see it he had built the most exacting method yet devised in medicine. That method, and the certainty it conferred, became the foundation of a science. And within a decade the same man, hunting a cure, would break his own rules and pay for it in his patients' lives.
The captain of death
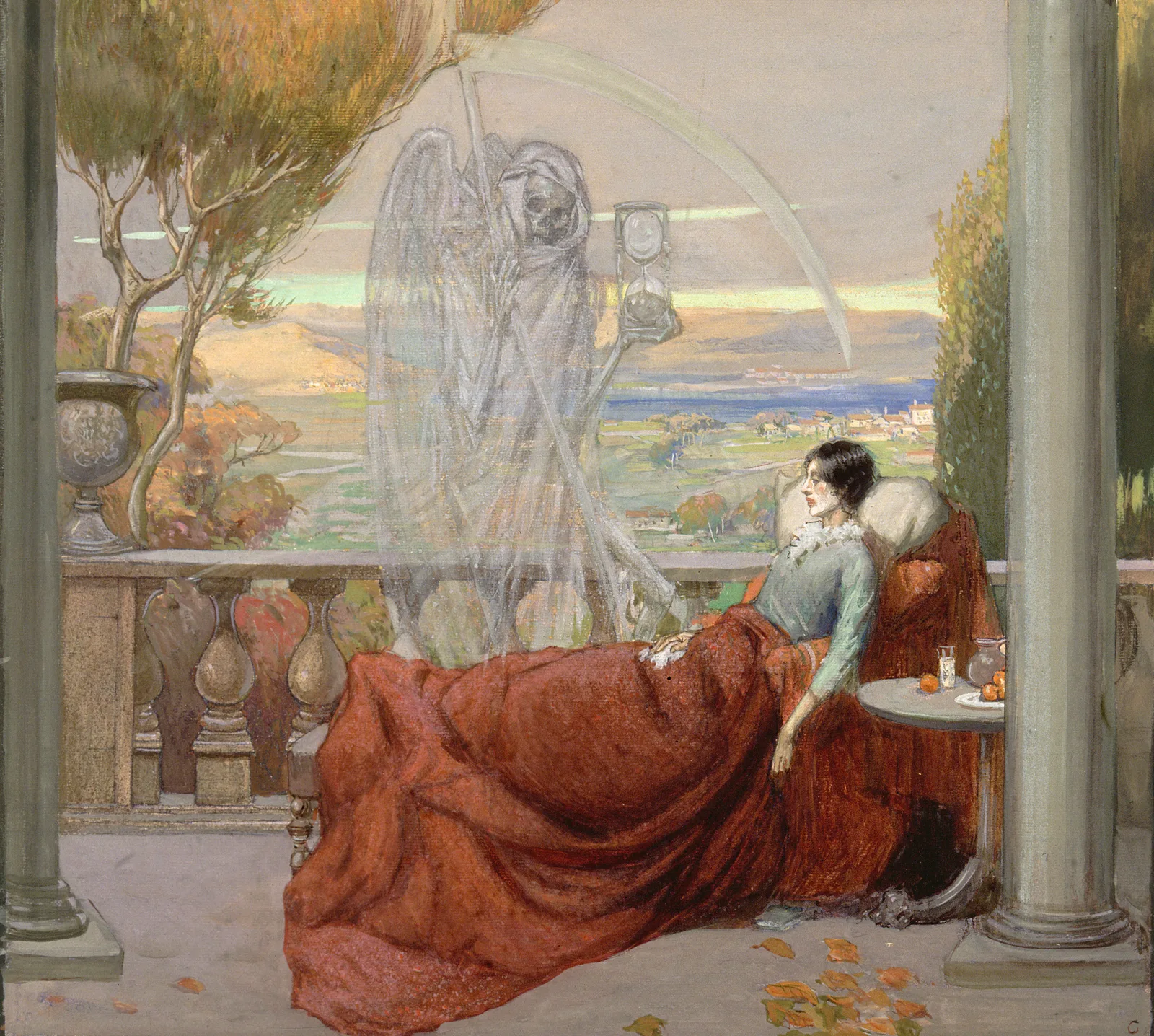
Tuberculosis in the nineteenth century was not one disease among many; it was the sea the others swam in. It went by a shelf of names (consumption, phthisis, the white plague, scrofula in the swollen glands of the neck) and in one form or another it accounted for something near a seventh of all deaths in Europe, and a far heavier share among the young adults it seemed to prefer.1 The disease had acquired a strange glamour by then, the wasting and the bright fevered eye read as marks of refinement, the consumptive poet coughing into a handkerchief half a literary type. What mattered more for medicine was that almost everyone believed the malady to be constitutional, an inherited weakness of the stock, a taint that ran in families and so could no more be caught than a squint could be caught.2 That consumption might be an infection, something passed from one person to another like a cold, was a minority opinion and a slightly vulgar one. The reigning view offered nothing to prevent and nothing to cure. It counselled mountain air, rich food, and resignation.
Making the invisible visible
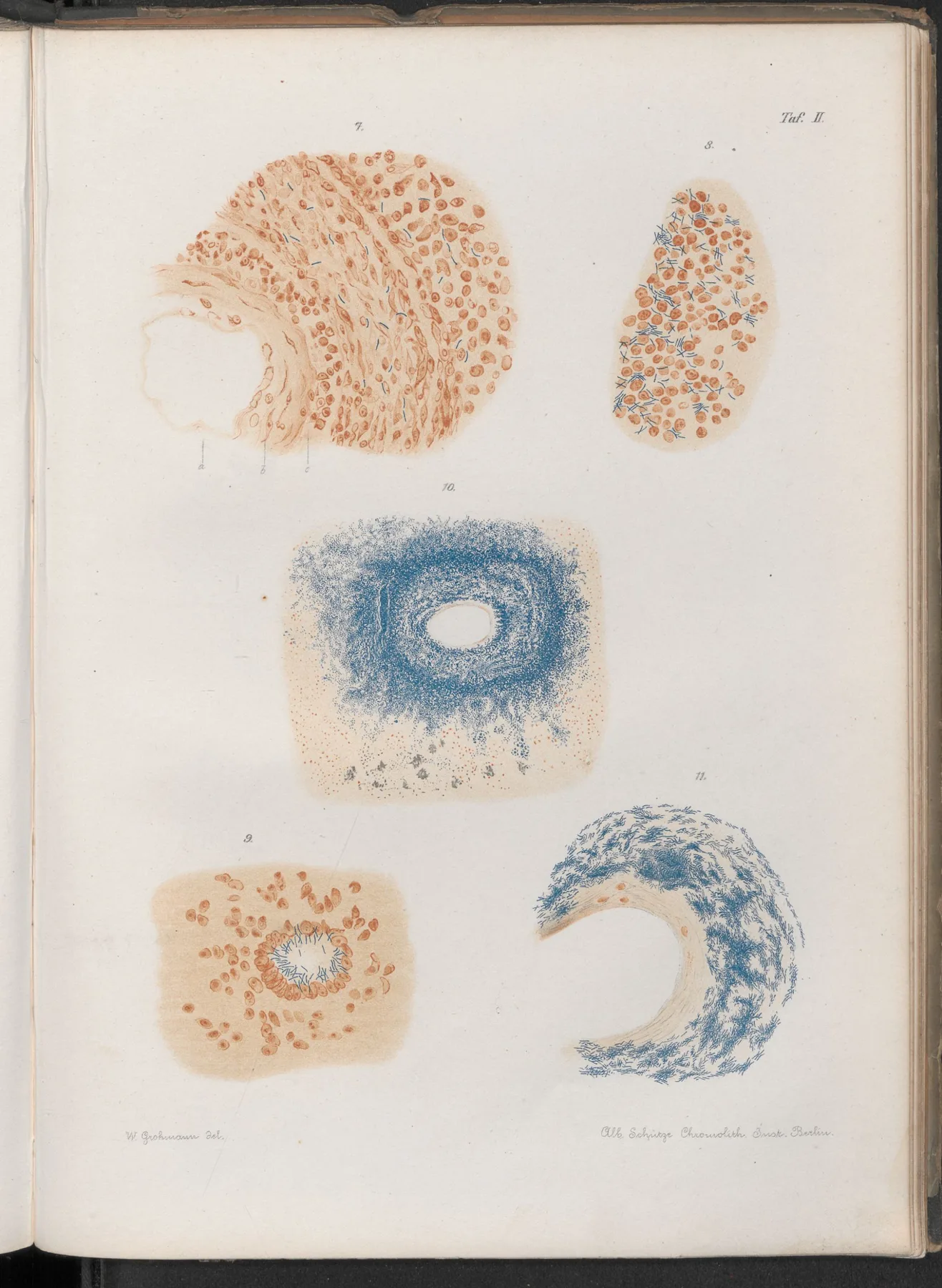
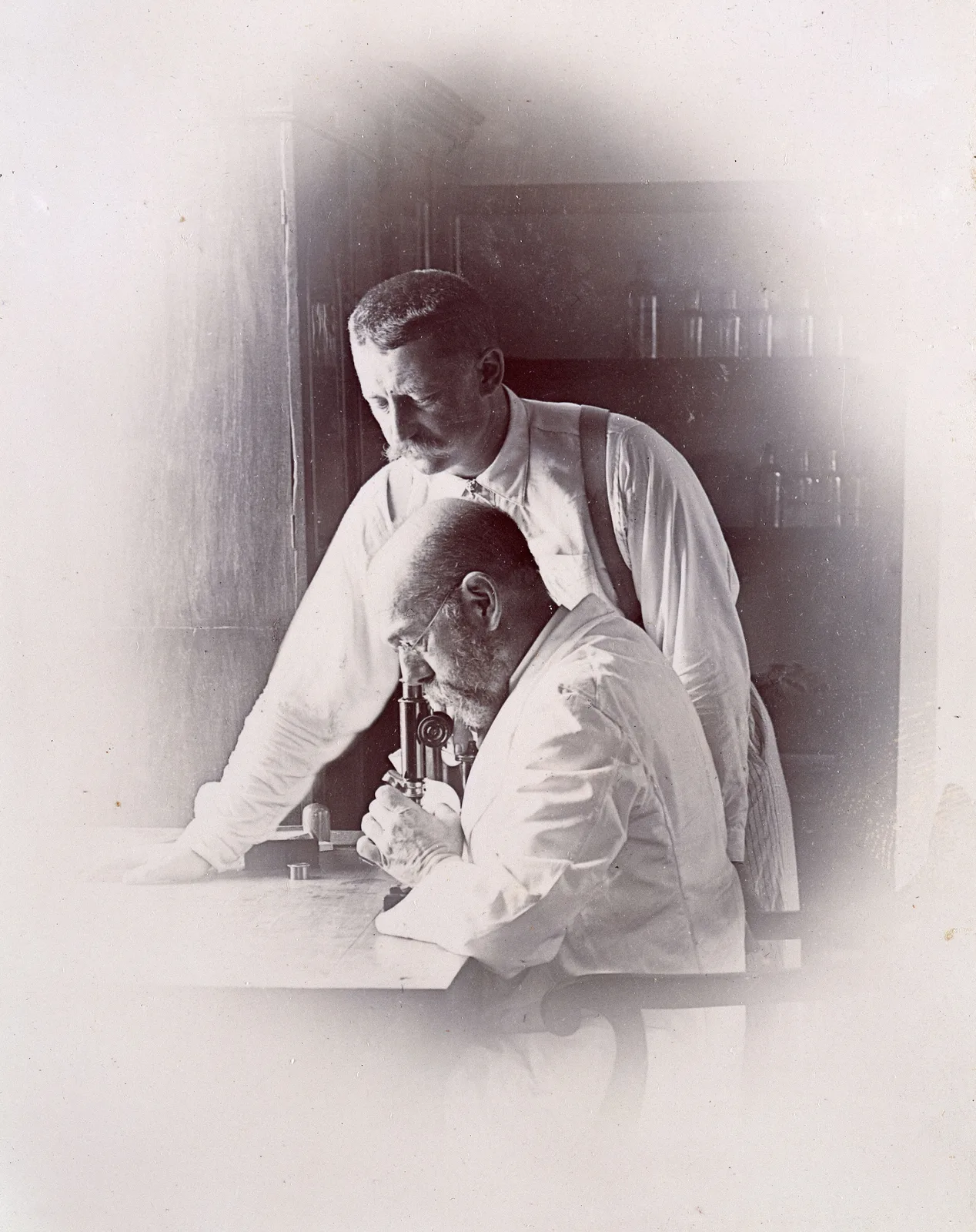
The man who overturned it was an unlikely revolutionary. Robert Koch was a district medical officer in a small town in the Prussian province of Posen, working in a laboratory he had partitioned off his consulting room with a curtain, largely self-taught, and already known for having pieced together the whole life cycle of the anthrax bacillus in that domestic set-up.3 Tuberculosis was a far harder quarry, for its organism is among the most retiring in all of pathology: exceptionally thin, sheathed in a waxy coat that shrugs off the watery dyes which stain other bacteria, and so scarce in diseased tissue that it hides among the body's own cells. Koch's gift was above all a technical one. He worked out a laborious staining routine, a bath in alkaline methylene blue for hours and sometimes overnight, followed by a brown counterstain, that at last made the bacilli stand out as fine blue rods against a paler ground.4 He grew them, with enormous patience, on the solid surface of heat-set blood serum, where the colonies crept into sight only after weeks rather than the hours a common microbe needs. And he took that pure culture and inoculated guinea pigs, which sickened and died of tuberculosis, and from their organs he recovered the same rod once more. Presence, isolation, reproduction, recovery: the chain closed on itself, and on the evening of the twenty-fourth of March, 1882, he set it before the Berlin Physiological Society.5 Paul Ehrlich, sitting in the audience, went home and set to work on the stain, announcing a decisive improvement within weeks, and called that evening the greatest scientific experience of his life.
The rules of proof
What Koch had done for tuberculosis he now proposed to do for infection at large, and the manner of the proof came to matter as much as the fact. Out of the tuberculosis work, and the studies of anthrax and wound infection around it, he distilled a set of conditions a microbe must meet before it could be convicted of causing a disease: it must be present in every case; it must be isolated and grown in pure culture away from the body; that culture must reproduce the disease in a healthy animal; and the same organism must be recovered from that animal in turn.6 These are the postulates that carry his name, and they converted the loose analogies of germ theory into something a court might recognise, a standard of evidence. The core of the idea was not new even in 1882. Koch's own teacher at Göttingen, the anatomist Jacob Henle, had argued in 1840 that contagia were living things and had sketched almost precisely these criteria for proving it, at a moment when there was no earthly way to satisfy them.7 What the pupil added to the master was not the logic but the means, the stains and the plates and the pure cultures that turned a philosopher's demand into a laboratory routine. It is a pattern this series keeps meeting: the systematiser remembered as the seer.
Where the rules break
The postulates were barely written before their own author began turning up the exceptions, and the most unsettling came from his own hand. Pursuing cholera to Egypt and India in 1883 and 1884, Koch identified its comma-shaped bacillus; but he also found that same organism thriving in people who were entirely well, healthy carriers who harboured the germ and shed it without ever falling ill.8 That one observation cracked the first and most intuitive postulate, the demand that the organism be found only in the sick, for here it sat in the healthy. Other diseases refused even the second condition. The leprosy bacillus, identified by the Norwegian Armauer Hansen almost a decade before Koch's tubercle bacillus, could not be grown in culture at all, and cannot be to this day.9 Syphilis, typhus, and in time the entire invisible world of viruses would each defy the postulates in their own way. To his credit Koch did not defend the rules as scripture; once the carriers appeared he loosened the first himself.10 Yet the deepest crack was already there in tuberculosis, the very disease that had seemed to vindicate the method most completely, and it would take a hundred years to see how wide it ran.
The secret remedy
Fame did to Koch what it has done to many, persuading him that his intuitions no longer needed proving. In the summer of 1890, at the Tenth International Medical Congress in Berlin, he let it be known that he had found a substance able to arrest tuberculosis, and by the autumn he was giving it, a glycerine extract of the bacilli he called tuberculin, to desperate patients who poured into the city from across Europe.11 He would not say what it contained. The secrecy was deliberate, tangled up with hopes of a patent, of profit, of an institute of his own, and it betrayed the very ethic of open proof on which he had built his name. The results were not merely disappointing but lethal. Rudolf Virchow, dissecting those who had died under the treatment, showed early in 1891 that tuberculin could rouse quiet disease into fatal activity rather than heal it, and the mounting deaths in the Berlin clinics turned a miracle into a scandal inside a few months.12 As a cure tuberculin failed utterly. Its afterlife is the sharpest irony of the whole affair: injected in a minute dose into the skin, Koch's failed remedy raises a small hard swelling in anyone whose body has met the bacillus before, and in that guise, the tuberculin skin test, it became and remains one of the most widely used diagnostic tools in all of medicine.13 The cure that killed became the test that reveals.
Read from the Ward
The oddest sentence I say to a well person is that they are infected. A screening test comes back positive, a bleb of dye raised on the forearm or a tube of blood sent for one of the newer assays, and the patient feels perfectly well, has never knowingly been ill, and yet somewhere inside them, most often walled into the apex of a lung, a colony of Koch's bacillus has been living quietly, sometimes for decades, held in check but never killed.14 Roughly a quarter of all the people alive carry the organism in this silent way. The great majority will go to their graves untroubled by it; somewhere between five and ten in a hundred will, at some point, have it wake.
This is the fact Koch's beautiful method could not hold. His first postulate asked that the germ be found in the sick; tuberculosis, in its commonest form by far, is the germ present in the well. The bacillus is necessary for the disease and nowhere near sufficient for it, and what decides whether a silent infection ever becomes a fatal one is less the microbe than the ground it lodges in: the age of the host, the hunger, the diabetes, the failing immunity. I meet the point of the exception most sharply where I work. The patients in whom a latent infection wakes and turns to meningitis, or seeds itself through the body like sown grain, are so often the very ones whose defences we have lowered ourselves — the transplant recipient, the patient on a drug that blocks one arm of the immune response, the person with untreated HIV. The germ had been there all along, keeping Koch's postulate waiting. We supplied the missing half of the equation.
Medicine has made its peace with the exceptions by loosening the rules. We speak now of molecular postulates, of meeting Koch's demand with a gene sequence in place of a whole cultured organism, of pathogens we can read letter by letter but have never grown in a dish.15 It is a humbler standard than the one he set that evening in 1882, and it has to be, because the living world proved more tangled than a clean chain of proof from a guinea pig. Even so, I would not want to work without the old rigour beneath me. When I treat a latent infection I have never seen, in a patient who has no symptoms, on the strength of a test descended from Koch's own failed cure, I am trusting a named and specific organism to behave in a specific way. That is his faith exactly, only held a little more loosely.
So I go on ordering the test he left us, a hundred times a year, and reading the small hard swelling three days later. When it is raised I tell a well person that something is alive in them, and that we will treat it before it can wake. It is at once the most Koch-like thing I do and the least: a specific germ, named and hunted just as he taught, standing behind a disease that has not happened and, in all likelihood, never will. The rod he lifted into view in that Berlin room is still in us, in a quarter of us, waiting. Most of the time, waiting is the whole of what it does.
- Near the start of his 1882 lecture Koch set out the toll: "One in seven of all human beings dies from tuberculosis. If one only considers the productive middle-age groups, tuberculosis carries away one-third, and often more." Robert Koch, "Die Aetiologie der Tuberculose," Berliner Klinische Wochenschrift 19 (1882): 221–30; on nineteenth-century mortality, Thomas Dormandy, The White Death: A History of Tuberculosis (London: Hambledon, 1999).↩
- On the constitutional/hereditary understanding of consumption and its Romantic image before 1882, see Dormandy, The White Death; and Helen Bynum, Spitting Blood: The History of Tuberculosis (Oxford, 2012).↩
- On Koch as district officer at Wollstein, the curtained home laboratory, and the anthrax life-cycle work (1876), see Thomas D. Brock, Robert Koch: A Life in Medicine and Bacteriology (Berlin: Springer, 1988).↩
- On Koch's methylene-blue-and-counterstain method for the tubercle bacillus and the difficulty of staining it, see Koch, "Die Aetiologie der Tuberculose" (1882); Brock, Robert Koch.↩
- On the solid coagulated-serum medium, the guinea-pig inoculations, the 24 March 1882 lecture to the Berlin Physiological Society, and Paul Ehrlich's presence and prompt improvement of the stain, see Brock, Robert Koch; Christoph Gradmann, Laboratory Disease: Robert Koch's Medical Bacteriology (Baltimore: Johns Hopkins University Press, 2009).↩
- The postulates in the form given here draw on Koch's tuberculosis and cholera papers and his 1890 address to the Tenth International Medical Congress; a fourth clause (re-isolation) is often added by later convention. See K. Codell Carter, "Koch's Postulates in Relation to the Work of Jacob Henle and Edwin Klebs," Medical History 29 (1985): 353–74.↩
- Jacob Henle, Von den Miasmen und Contagien und von den miasmatisch-contagiösen Krankheiten (Berlin, 1840); Henle taught Koch at Göttingen, and the criteria are often called the Henle–Koch postulates. See Carter, "Koch's Postulates" (1985).↩
- On the 1883–84 cholera expedition, the comma bacillus, and Koch's recognition of healthy carriers, see Brock, Robert Koch; Gradmann, Laboratory Disease.↩
- Mycobacterium leprae was identified by Gerhard Armauer Hansen in 1873 and has never been cultivated on artificial media; it is propagated only in living hosts. See Brock, Robert Koch.↩
- On Koch's own qualification of the first postulate after the carrier findings, see Carter, "Koch's Postulates" (1985); Alfred S. Evans, "Causation and Disease: The Henle–Koch Postulates Revisited," Yale Journal of Biology and Medicine 49 (1976): 175–95.↩
- On the August 1890 announcement at the Tenth International Medical Congress, the secret glycerine extract ("tuberculin"), and the commercial and institutional motives behind the secrecy, see Christoph Gradmann, "Robert Koch and the Pressures of Scientific Research: Tuberculosis and Tuberculin," Medical History 45 (2001): 1–32.↩
- Rudolf Virchow reported autopsies of tuberculin-treated patients to the Berlin Medical Society early in 1891, showing the agent could activate rather than heal disease; on the ensuing deaths and scandal, see Gradmann, "Robert Koch and the Pressures of Scientific Research" (2001).↩
- On tuberculin's reinvention as a diagnostic — von Pirquet's cutaneous test (1907) and Mantoux's intradermal method (1908), later standardised as the purified protein derivative (PPD) skin test — see the historical summary in Brock, Robert Koch, and standard tuberculosis references.↩
- On the global prevalence of latent tuberculosis infection at roughly one-quarter of humanity (about 1.7 billion), see Rein M. G. J. Houben and Peter J. Dodd, "The Global Burden of Latent Tuberculosis Infection: A Re-estimation Using Mathematical Modelling," PLoS Medicine 13 (2016): e1002152. The 5–10 per cent lifetime risk of reactivation is the standard World Health Organization estimate; see WHO, Latent Tuberculosis Infection: Updated and Consolidated Guidelines for Programmatic Management (Geneva: WHO, 2018).↩
- On the reformulation of the postulates for the molecular age, see Stanley Falkow, "Molecular Koch's Postulates Applied to Microbial Pathogenicity," Reviews of Infectious Diseases 10, suppl. 2 (1988): S274–76; and David N. Fredricks and David A. Relman, "Sequence-Based Identification of Microbial Pathogens: A Reconsideration of Koch's Postulates," Clinical Microbiology Reviews 9 (1996): 18–33.↩
- Brock, Thomas D. Robert Koch: A Life in Medicine and Bacteriology. Berlin: Springer, 1988.
- Bynum, Helen. Spitting Blood: The History of Tuberculosis. Oxford: Oxford University Press, 2012.
- Carter, K. Codell. "Koch's Postulates in Relation to the Work of Jacob Henle and Edwin Klebs." Medical History 29 (1985): 353–74.
- Dormandy, Thomas. The White Death: A History of Tuberculosis. London: Hambledon Press, 1999.
- Fredricks, David N., and David A. Relman. "Sequence-Based Identification of Microbial Pathogens: A Reconsideration of Koch's Postulates." Clinical Microbiology Reviews 9 (1996): 18–33.
- Gradmann, Christoph. Laboratory Disease: Robert Koch's Medical Bacteriology. Baltimore: Johns Hopkins University Press, 2009.
- Gradmann, Christoph. "Robert Koch and the Pressures of Scientific Research: Tuberculosis and Tuberculin." Medical History 45 (2001): 1–32.
- Houben, Rein M. G. J., and Peter J. Dodd. "The Global Burden of Latent Tuberculosis Infection: A Re-estimation Using Mathematical Modelling." PLoS Medicine 13 (2016): e1002152.