The cylinder was the easy part. What Laennec did with it over the ten years left to him was harder and stranger: he taught the living body to testify. He listened to the dying and set down every sound a chest could make; then he opened the dead and found the lesion that had made each one, and matched the two until a noise could stand for a thing no eye had seen. He had to find words for them as he went, for the sounds had never been named. And in the naming he quietly changed what a disease was, and whose account of it a physician was bound to trust.
The closed country
For as long as medicine had existed, the inside of a living person was a country closed to the physician. He could see the surface, take the pulse, watch the breath, read the colour of the skin and the white of the eye; past that he depended on what the patient could tell him. Disease announced itself as a story of a chill, a pain that wandered, a cough grown worse by night, and the physician's art was the art of construing that story.1 The interior gave up its secrets only on the table of the dead, too late to help the man who had owned it. What a patient suffered and what had gone wrong inside him were two accounts, and only the first was available in life.
That older medicine understood illness as something belonging to the whole person. A fever was an imbalance spread through the body, a disturbance of its humours, not a lesion lodged in one organ while its neighbour went free. To know the seat of a disease you waited for the autopsy, and by then the question had answered itself in the worst way.
The wooden tube Laennec turned on a lathe in the autumn of 1816 cracked that closed country open.2 Its making is remembered as the birth of the stethoscope, a story told elsewhere. What is easy to forget is that the instrument by itself disclosed nothing: a cylinder held to a chest delivers only a confusion of noise to an ear that cannot read it. The achievement that mattered came after, and took the rest of a short life.
The sound and the lesion
Laennec had been schooled to think of disease as a thing with a location. His Paris was the city of Bichat, who had taught that the body's diseases settle not in organs only but in the tissues that compose them, and of Gaspard Bayle, his own teacher, who had sat among the consumptive and counted the lesions of phthisis in the dead.3 The habit of mind was already there. The cylinder gave it an ear.
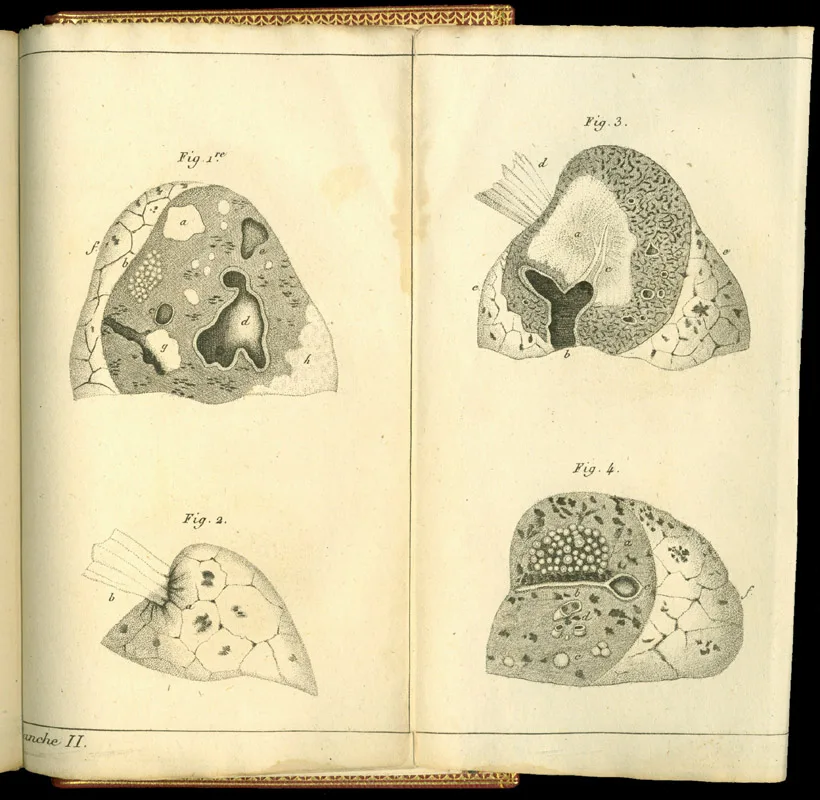
At the Hôpital Necker, Laennec set himself a labour of correlation that reads now like devotion. He listened to the living and wrote down precisely what he heard; and when the patient died, as so many on those wards did, he opened the chest and looked for the thing that had made the sound.4 He would not name a noise until he had seen, in the dead-house, the lesion beneath it. Over hundreds of such pairings a dictionary took shape, in which a sound caught through a foot of wood could be read as a ruin no eye would ever reach in the living. The great teacher in this was phthisis, the consumption quietly emptying the wards, whose cavities and rattlings Laennec learned to recognise in a patient who still sat up and answered him.
Words for what had no name
The sounds had never been named, for no one before had heard them clearly enough to need names. Laennec named them himself, coining some from the Greek and pressing older words into new service, and he did it with the plain ear of the Breton countryside he came from. The bubbling and rattling of fluid in the airways he first called the râle. The word gave him trouble at once. In French, râle carried a shadow it carries still: le râle de la mort, the death rattle, the noise of a man who can no longer clear his own throat.5 Laennec could not stand over a frightened patient and pronounce, to the listening family, the very sound of dying. So for the bedside he offered a borrowed word: rhonchus, a snore, the Latin synonym a physician could pronounce in front of a frightened patient.6 The double naming bred a confusion that a century of physicians never fully untangled.
The others followed, each tied to a thing he had heard and then seen. Crepitation, the fine dry crackle he likened to a pinch of salt thrown on a hot plate. Egophony, from the goat: the thin, bleating, nasal quaver the voice takes on as it crosses a shallow layer of fluid, a sound he learned to find just above an effusion.7 Pectoriloquy, the chest speaking, the spoken voice ringing strangely clear and close through the wall, which meant a cavity had been hollowed in the lung beneath. Bronchophony for its lesser cousin. The instrument could be turned out by any carpenter for a few sous. The vocabulary could only be earned, one body at a time, and it was the vocabulary that was the discovery.
From the story to the sign
He gathered the whole of it into a treatise in 1819, De l'auscultation médiate, and was still revising it when he died, the second edition appearing in the year of his death.8 Within two years it had crossed the Channel. John Forbes, a Scottish physician who had got hold of one of the new cylinders, put Laennec into English in 1821 and carried auscultation to Britain; the book ran to four editions in his hands.9 Forbes thought the French names clumsy and altered several as he translated, seeding Laennec's râle and rhonchus muddle in two languages at once.
Something larger than a vocabulary had shifted. Medicine had always taken its first evidence from the symptom, which is what the patient reports and what only the patient can feel. Laennec's signs were a different order of thing: they were present whether or not the sufferer knew it, and a stranger's trained ear could go in and find them.10 Disease came loose from the patient's account and fastened instead to a place, a lesion in an organ, which the living chest would now give up under examination. Later historians have called this the birth of the clinical gaze, the moment the physician's attention began to travel past the person toward the part.11 Something real was won that has never been handed back, the cavity heard before it could be seen. Something quieter was surrendered. The patient slowly ceased to be the one who told the doctor what was wrong, and became the body in which the doctor found it.
One sound, one lesion?
The dictionary was a beautiful idea, and perhaps a shade too beautiful. Its promise was that each sound betrayed one lesion, cleanly, the way a word names one thing. The lungs were less obedient than that. In Vienna, a generation on, Josef Škoda rebuilt the catalogue on physical principles, classing the sounds by pitch and resonance rather than by the diseases Laennec had tied them to, and arguing that one note might rise from quite different states of the chest.12 The sign, in other words, was a likelihood and not a proof. Laennec himself, listening for what he already expected, now and then heard more in a sound than was truly in it; the best of his successors took his signs as evidence to be weighed, never as verdicts.
There was a harder limit still. All this exquisite hearing transformed what could be known and left almost untouched what could be done. Phthisis, whose every cavity and crackle Laennec could now name in a man still walking and talking, killed as reliably after 1819 as before it. It killed Laennec himself, ten years on, in a chest his own nephew sounded with his own instrument.13 To hear a disease with perfect clarity and be powerless to halt it is a particular kind of knowledge, and the bedside has been learning to carry it ever since.
Reading the silent
Most of my patients cannot tell me what is wrong. They come to me intubated, or sedated, or struck dumb by a stroke, or sunk past the reach of any question into coma. Medicine's first witness, the patient's own account of himself, is precisely the one I am most often denied. What I am left with is the body and the signs it gives off without consent: the rhythm of the breathing, the width of a pupil, the way a lifted limb drops when I let it go. I spend my days reading people who cannot speak for themselves, and I read them, still, by the method Laennec worked out over the silent chests at Necker.
His discipline remains the spine of how I was trained. The neurological examination is auscultation by another route, a catalogue of signs drawn out of a body that may say nothing, each one matched in the mind to a lesion in a place. From the pattern I name the level of the cord, the territory of the blocked artery; then the scan, the distant grandchild of Röntgen's ray, tells me whether I read the body rightly. That loop between the sign and the lesion, neither one trusted quite alone, is the whole of clinical diagnosis, and it is Laennec's loop exactly, run now in hours instead of at the autopsy table.
And here the modern temptation walks in. The image hands me the lesion directly, drawn cleaner than any dissection Laennec performed, and beside it the laid-on hand and the listening ear can feel like courtesies owed to an older age. I think that gets the matter backwards. The picture shows me structure; the sign shows me function, what the living body is doing with its injury at this hour, which no still image holds. And Škoda's old caution stands at my shoulder whenever I am too pleased with a finding: one sign need not mean one disease. The body offers likelihoods, and asks me to weigh them, exactly as it asked him.
Last week I stood over a man who could not answer a single question I put to him, and I did the unremarkable thing. I warmed the bell of the same two-century-old instrument in my hand, and laid it to his chest, and went quiet, and listened. There was nothing modern in the act, and nothing in it Laennec would not have recognised: a physician bent over a body that could not testify in any language but the one he taught us to hear. Whether a cure follows is never wholly in my gift. The listening comes first, and it still falls to a person to do it.
Read from the Ward
Most of my patients cannot tell me what is wrong. They come to me intubated, or sedated, or struck dumb by a stroke, or sunk past the reach of any question into coma. Medicine's first witness, the patient's own account of himself, is precisely the one I am most often denied. What I am left with is the body and the signs it gives off without consent: the rhythm of the breathing, the width of a pupil, the way a lifted limb drops when I let it go. I spend my days reading people who cannot speak for themselves, and I read them, still, by the method Laennec worked out over the silent chests at Necker.
His discipline remains the spine of how I was trained. The neurological examination is auscultation by another route, a catalogue of signs drawn out of a body that may say nothing, each one matched in the mind to a lesion in a place. From the pattern I name the level of the cord, the territory of the blocked artery; then the scan, the distant grandchild of Röntgen's ray, tells me whether I read the body rightly. That loop between the sign and the lesion, neither one trusted quite alone, is the whole of clinical diagnosis, and it is Laennec's loop exactly, run now in hours instead of at the autopsy table.
And here the modern temptation walks in. The image hands me the lesion directly, drawn cleaner than any dissection Laennec performed, and beside it the laid-on hand and the listening ear can feel like courtesies owed to an older age. I think that gets the matter backwards. The picture shows me structure; the sign shows me function, what the living body is doing with its injury at this hour, which no still image holds. And Škoda's old caution stands at my shoulder whenever I am too pleased with a finding: one sign need not mean one disease. The body offers likelihoods, and asks me to weigh them, exactly as it asked him.
Last week I stood over a man who could not answer a single question I put to him, and I did the unremarkable thing. I warmed the bell of the same two-century-old instrument in my hand, and laid it to his chest, and went quiet, and listened. There was nothing modern in the act, and nothing in it Laennec would not have recognised: a physician bent over a body that could not testify in any language but the one he taught us to hear. Whether a cure follows is never wholly in my gift. The listening comes first, and it still falls to a person to do it.
- On the pre-auscultatory clinic, in which diagnosis rested on the patient's reported symptoms and a humoral conception of disease as a disturbance of the whole person rather than a localised lesion, see Stanley Joel Reiser, Medicine and the Reign of Technology (Cambridge: Cambridge University Press, 1978), chap. 1; Michel Foucault, The Birth of the Clinic: An Archaeology of Medical Perception, trans. A. M. Sheridan (London: Tavistock, 1973).↩
- On the 1816 invention of the wooden cylinder at the Hôpital Necker, recounted at length in the companion plate, see R. T. H. Laennec, De l'auscultation médiate (Paris: Brosson et Chaudé, 1819), preface; Jacalyn Duffin, To See with a Better Eye: A Life of R. T. H. Laennec (Princeton: Princeton University Press, 1998).↩
- On the anatomical context — Xavier Bichat's pathology of the tissues and Gaspard-Laurent Bayle's clinicopathological study of phthisis, under which Laennec was formed — see Duffin, To See with a Better Eye; Foucault, The Birth of the Clinic.↩
- On Laennec's anatomo-clinical method at Necker, correlating sounds heard in the living with lesions found at post-mortem, see Duffin, To See with a Better Eye; Reiser, Medicine and the Reign of Technology.↩
- On râle and its everyday French sense of the death rattle, le râle de la mort, and Laennec's consequent unease with the word at the bedside, see A. J. Robertson and R. Coope, "Râles, Rhonchi, and Laennec," The Lancet 270, no. 6992 (1957): 417–23; R. T. H. Laennec, De l'auscultation médiate, 2nd ed. (Paris: J.-S. Chaudé, 1826), preface.↩
- On Laennec's offering of the Latin rhonchus (a snore) as a synonym to be spoken in front of patients, and the lasting muddle between the two terms in French and English, see Robertson and Coope, "Râles, Rhonchi, and Laennec"; A. Sakula, "R T H Laennec 1781–1826: His Life and Work: A Bicentenary Appreciation," Thorax 36, no. 2 (1981): 81–90.↩
- On the principal signs — crepitation, egophony (the goat-like bleating of the voice heard above a pleural effusion), pectoriloquy (the voice ringing through a pulmonary cavity) and bronchophony — and Laennec's homely analogies for them, see Laennec, De l'auscultation médiate (1819); Roguin, "The Man Behind the Stethoscope."↩
- R. T. H. Laennec, De l'auscultation médiate, ou Traité du diagnostic des maladies des poumons et du cœur, 1st ed. (Paris: Brosson et Chaudé, 1819); 2nd ed., revised and retitled Traité de l'auscultation médiate et des maladies des poumons et du cœur (Paris: J.-S. Chaudé, 1826).↩
- On John Forbes's English translation, A Treatise on Diseases of the Chest (London: T. & G. Underwood, 1821); its four editions to 1834 (the second, 1827, retitled to add and on Mediate Auscultation); and his much-criticised alteration of Laennec's terminology, see "John Forbes FRS (1787–1861)," James Lind Library; Sakula, "Laennec 1781–1826."↩
- On the shift from symptom (reported by the patient) to physical sign (elicited by the examiner) as the primary evidence of disease, see Reiser, Medicine and the Reign of Technology, chap. 1.↩
- On the "anatomo-clinical method" and the "clinical gaze" as the threshold of modern medical perception, an interpretation due to Michel Foucault, see The Birth of the Clinic; for the rise of the clinicopathological method in early-nineteenth-century France more broadly, see the history-of-medicine literature on morbid anatomy.↩
- On Josef Škoda, Abhandlung über Perkussion und Auskultation (Vienna: J. G. Ritter von Mösle's Witwe & Braumüller, 1839), reclassifying auscultatory sounds by their physical qualities of pitch and tone and loosening Laennec's strict one-sound-one-lesion correspondence, see Sakula, "Laennec 1781–1826"; "Joseph Skoda," history-of-medicine eponym literature.↩
- On Laennec's death from cavitary pulmonary tuberculosis in August 1826, examined in his last illness by his nephew Mériadec with the instrument he had devised, see Roguin, "The Man Behind the Stethoscope"; Duffin, To See with a Better Eye.↩
- Laennec, R. T. H. De l'auscultation médiate, ou Traité du diagnostic des maladies des poumons et du cœur. Paris: Brosson et Chaudé, 1819. 2nd ed., retitled Traité de l'auscultation médiate et des maladies des poumons et du cœur, Paris: J.-S. Chaudé, 1826.
- Forbes, John, trans. A Treatise on Diseases of the Chest. By R. T. H. Laennec. London: T. & G. Underwood, 1821.
- Duffin, Jacalyn. To See with a Better Eye: A Life of R. T. H. Laennec. Princeton: Princeton University Press, 1998.
- Roguin, Ariel. "Rene Theophile Hyacinthe Laënnec (1781–1826): The Man Behind the Stethoscope." Clinical Medicine & Research 4, no. 3 (2006): 230–35.
- Sakula, A. "R T H Laennec 1781–1826: His Life and Work: A Bicentenary Appreciation." Thorax 36, no. 2 (1981): 81–90.
- Robertson, A. J., and R. Coope. "Râles, Rhonchi, and Laennec." The Lancet 270, no. 6992 (1957): 417–23.
- Reiser, Stanley Joel. Medicine and the Reign of Technology. Cambridge: Cambridge University Press, 1978.
- Foucault, Michel. The Birth of the Clinic: An Archaeology of Medical Perception. Translated by A. M. Sheridan. London: Tavistock, 1973.
- Škoda, Josef. Abhandlung über Perkussion und Auskultation. Vienna: J. G. Ritter von Mösle's Witwe & Braumüller, 1839.