The most famous photograph in the history of medicine is a woman's hand, the finger-bones pale and a wedding ring hanging dark upon them. It is remembered as the moment medicine learned to see. Read a second time, it is also a bill. The ring is dark because it drank the rays that passed so lightly through her flesh, and whatever the new ray did not pass through cleanly, it spent itself upon. Within a year the same ray was being aimed, on purpose, to burn. The shadow it cast fell not only across the plate but down the length of lives not yet lived.
What stops the ray pays for it
Röntgen's picture is legible for a single reason: matter that stops the ray shows bright, and matter that lets it pass shows dark, so that bone stands out against flesh and metal stands out against bone.1 A radiograph is a map of what each tissue took from the beam. And the energy a tissue takes from the beam is dose, deposited in the flesh the rays cross on their way through. The wedding ring is the darkest thing in the frame because it absorbed the most, and that absorption is the germ of the injury: the ray spends itself on whatever slows it, and what it spends is paid by the tissue in its path. The first image ever made by the rays already carried the principle of their danger, written in the same grey light that made them a marvel. No one read it that way for years. There was too much to see.
The ray turned round
It took less than a year for the ray to be turned from seeing to destroying. On the twenty-fourth of November 1896, in Vienna, a physician named Leopold Freund laid a five-year-old girl beneath an X-ray tube borrowed from a photographic institute and began to irradiate the great hairy mole that covered most of her back.2 He meant to make the hair fall out, and it did. It was the first therapeutic use of the new rays to be documented and proved, and Freund is remembered as the founder of radiotherapy. What is less often told is the rest of the girl's story. To satisfy himself that the effect came from the rays and not from the electrical apparatus, Freund gave a second, longer course to her lower back; the hair fell away there too, and in its place opened an ulcer that took six years to heal and left her scarred for life.3 The first triumph of the treatment and its first grave wound were the same course of exposures, on the same small back.
Others were turning the ray on tumours that same year. In the Savoie that summer, the Lyon-trained physician Victor Despeignes turned the rays on a man's cancer of the stomach and published the first medical paper on X-ray therapy; in Chicago, Emil Grubbé claimed to have treated a woman's breast cancer that January, though no contemporaneous record survives to prove it.4 The first clearly successful cures came a little later, in Stockholm, where Tage Sjögren and Thor Stenbeck cleared skin cancers by long, patient courses, Stenbeck taking ninety-nine separate sessions over a single basal-cell carcinoma.5 The ray could cut without a knife. It could also, in the same motion, cut what ought to have been left alone.
A dose the colour of a pastille
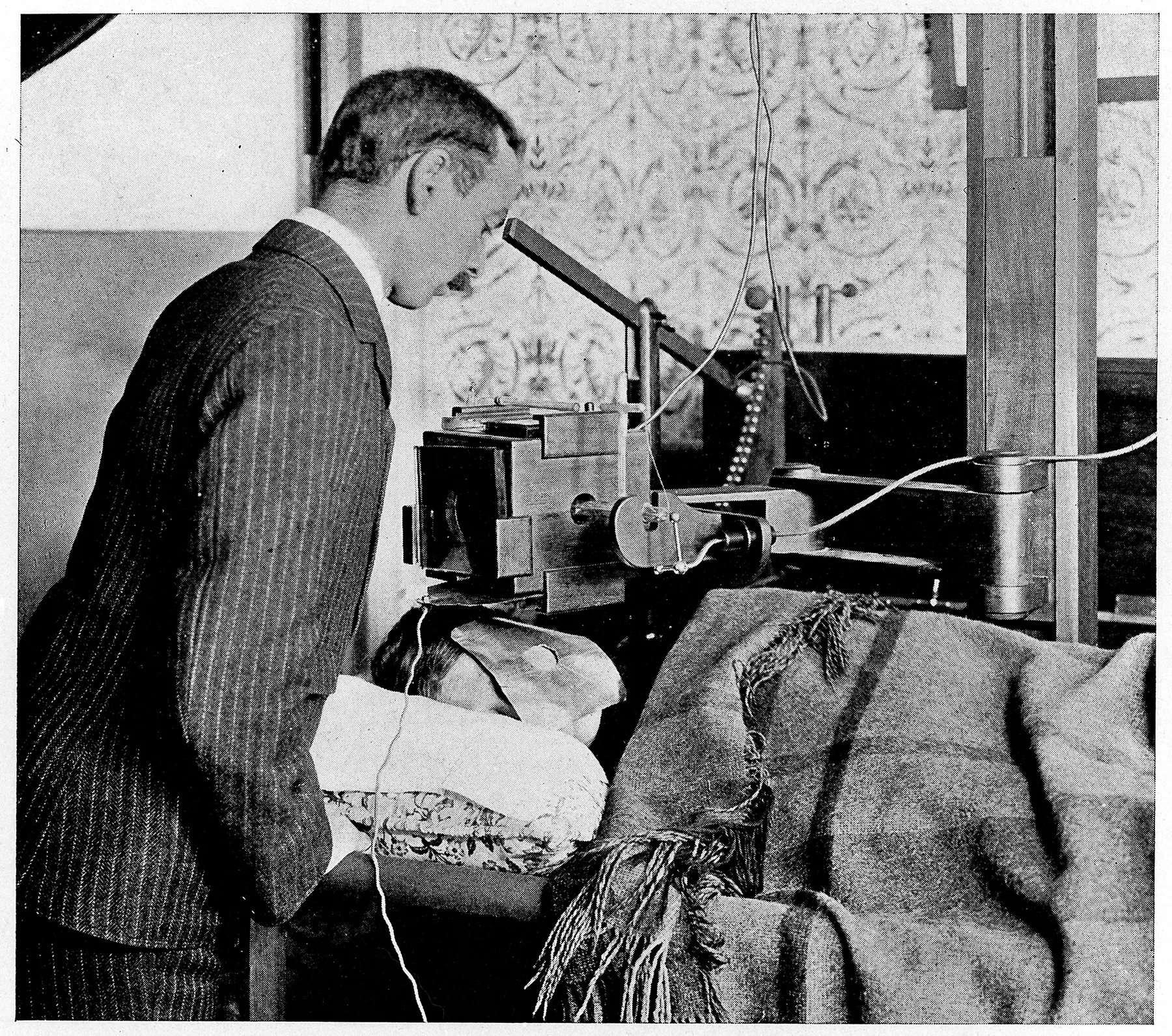
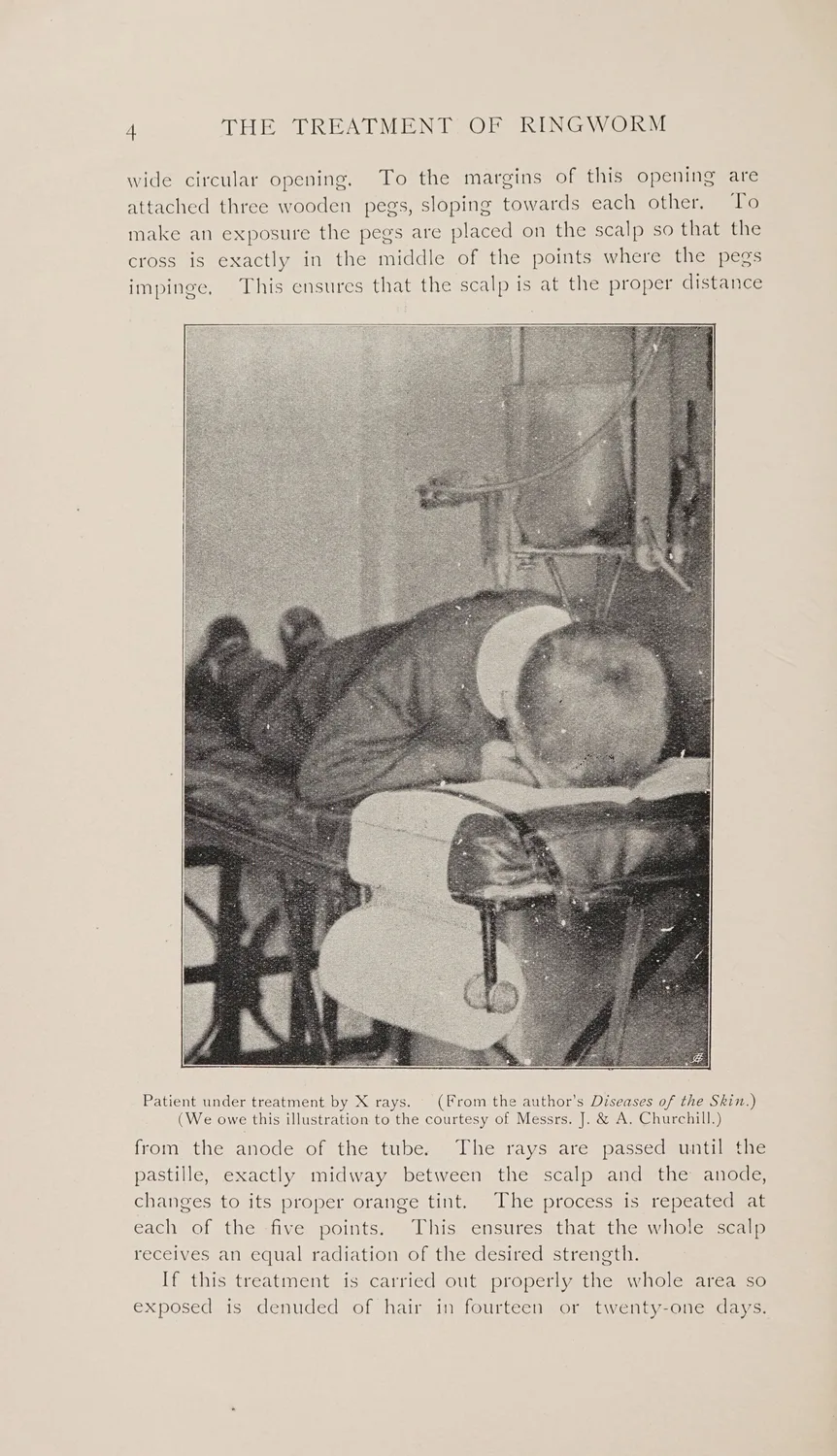
The trouble was that no one could yet say how much ray they were giving. There was no unit. In the first years the only gauge of dose was the body's own response: the operator judged an exposure by how red the skin became, the same crude reckoning by which the early radiologists had burned their hands.6 For treatment this was worse than imprecise, because the reddening came late, when the dose had already been delivered. In 1904 two Frenchmen, Raymond Sabouraud and Henri Noiré, offered a small improvement, a pastille of barium platinocyanide that changed colour under the rays, laid on the patient's skin so that the operator need not redden his own.7 When the pastille reached a particular shade, tint B on their scale, a full dose had been laid on the skin, and the heavier dose that would shed the hair was read from the same band of colour. A generation of medicine set the dose to a child's scalp by matching a colour to a chip on a card.
The children's hair
The reason a scale for the epilating dose mattered so much was ringworm. Tinea capitis, a fungal infection of the scalp, ran through the crowded schools and orphanages and immigrant quarters of the early twentieth century, and it was miserable to treat, because the fungus sheltered in the hair follicles where ointments could not reach. X-rays offered an elegant solution: irradiate the scalp in overlapping fields until every hair loosened and fell, carry the fungus off with it, and let the hair grow back clean.8 It worked. Across the first half of the century hundreds of thousands of children had their heads irradiated for ringworm, in Europe, in America, and, most systematically, in the new state of Israel, where an estimated twenty thousand children were treated in a national campaign between 1948 and 1960.9
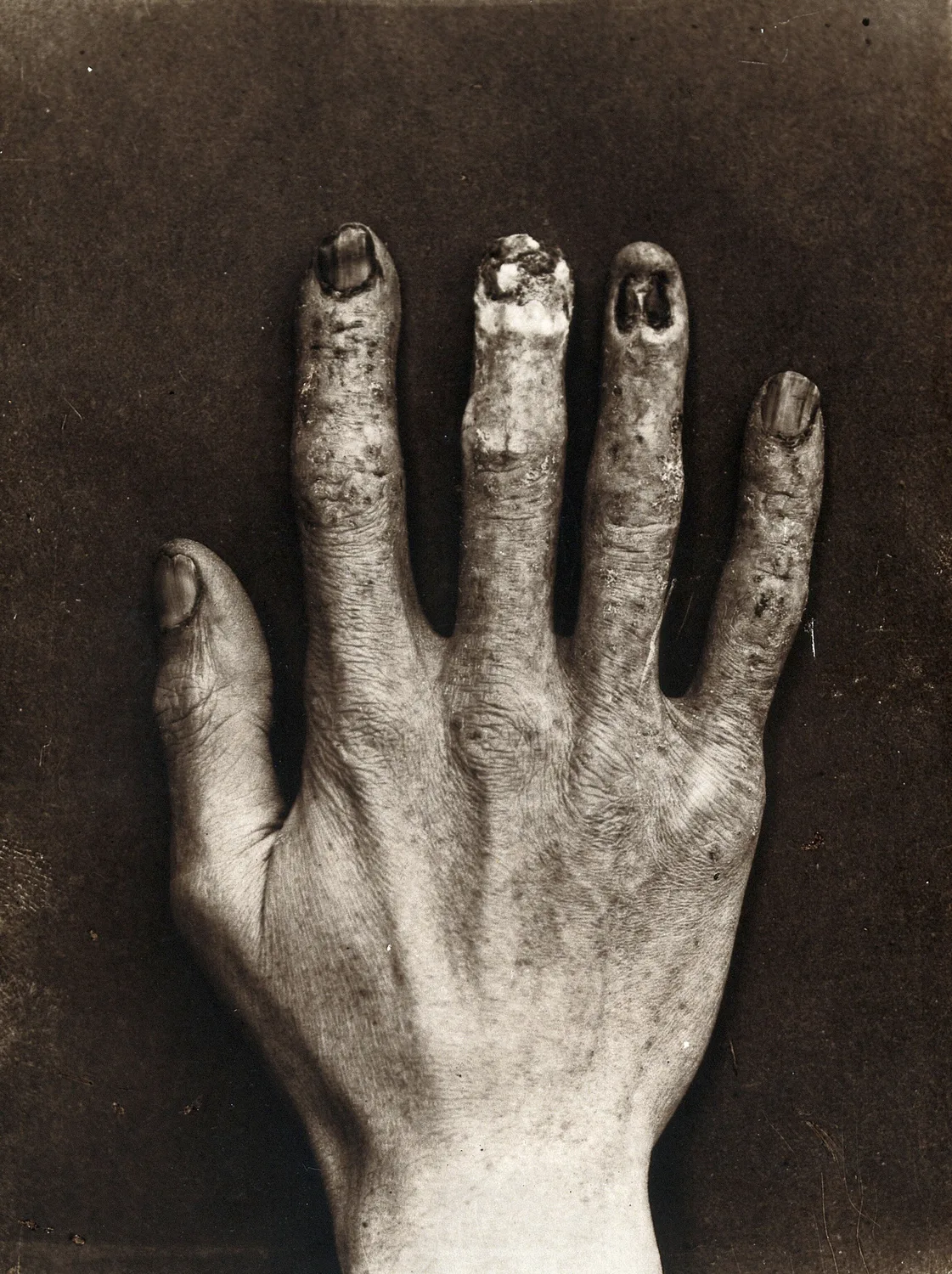
The hair grew back. The dose stayed. When those children were followed into middle age, the irradiated scalps were found to have delivered a real dose to the brain and thyroid beneath, and the cohorts carried, decades on, a distinct excess of meningiomas, other brain tumours, thyroid cancers, and skin cancers of the head and neck.10 They had been treated, as children, for a nuisance of the scalp, and the bill arrived forty years later, in the tissue the beam had crossed on its way to the hair. This is the ray's particular cruelty, the same one that had taken the radiologists' hands: it renders no receipt at the moment of the charge, and it is patient.
The marvel in the shoe shop
If medicine dosed children for disease, commerce dosed them for the fun of it. From the 1920s a device called the shoe-fitting fluoroscope stood in shoe shops across America and Europe (some ten thousand in the United States alone), a wooden cabinet with an X-ray tube in its base and three viewing hoods in its top.11 A customer put their feet in the slot and looked down at their own bones wriggling in green fluorescent light, the salesman and the child's mother watching through the other two hoods. It was marketed above all for children, whose growing feet were said to need the closest fitting, and a restless child might be stood on the machine several times in a single visit. Even a routine look gave the feet far more radiation than the fit of a shoe could be worth, and the worst machines could put close to a gray into them at a single stand.12 The harm was already known, for the first radiologists had died of it, and still the machines stood in the shops for the better part of fifty years, until warnings in the 1950s and a slow procession of bans, beginning with Pennsylvania in 1957, at last emptied them out in the early 1970s.13

Learning to weigh the light
What finally disciplined the ray was the slow invention of a way to measure it. In 1925 a physicist named Arthur Mutscheller proposed the first tolerance dose (a rate of exposure a worker might absorb, he judged, without harm) and set it at roughly a hundredth of the skin-reddening dose per month.14 It was a guess, but it was a numerical guess, and it moved the reckoning off the surface of the skin. Three years later, at the international radiology congress held in Stockholm in 1928, the profession at last agreed on a physical unit of exposure and named it the roentgen, after the man who had refused to put his name on anything.15 Dose could now be counted before it was felt. And in 1936 the German radiological society raised, in the garden of a Hamburg hospital, a monument to the X-ray and radium martyrs of all nations: a stone carved with the names of the doctors, nurses, and technicians the rays had killed. It bore a hundred and fifty-nine names when it was unveiled. By 1960 it held three hundred and fifty-nine, cut into further plaques as the profession went on burying its own.16
Read from the Ward
The scan on my screen this morning belonged to a woman of seventy-four, sent up for headaches, and it showed a meningioma: a smooth, benign, slow-growing mass sitting against the inner table of the skull, the commonest tumour of its kind. Nothing in the image was unusual. What stopped me was a single line in her history, taken down by a resident who cannot have known why it mattered. As a small girl, newly arrived in the country, she had been treated for ringworm of the scalp. I looked back at the smooth mass on the screen and understood that I might be reading, on a Tuesday morning three-quarters of a century later, the shadow of a ring of light laid on a child's head to make her hair fall out.
I cannot prove the connexion in her, and I did not try to. The single case keeps its silence; it is the twenty thousand behind her who speak. But standing at the screen I felt the particular vertigo of my trade, which is that the past does not stay past inside a body. A dose a physician gave in good faith in 1951, to cure a trivial thing, was still being paid down in the tissue in front of me.
The ray Freund turned on that first small back is still among the most powerful things medicine owns. We have not put it down; we have learned to weigh it. The beam once aimed by the reddening of skin is now shaped to the millimetre and metered in fractions of a gray, mapped onto the tumour and steered off everything around it, and the whole vast apparatus of modern radiation oncology exists to keep the ray on the disease and off the child. It is one of the quiet triumphs of the century, and it rests entirely on the thing the pioneers did not have and paid to give us: a number for the dose.
There is a stone in a hospital garden in Hamburg with three hundred and fifty-nine names on it, and blank surface left below the last of them. It was carved that way on purpose. The people who raised it understood that the list was not closed, that the ray collects on a delay, and that some of the names not yet cut belong to patients as much as to physicians. I think of that unfilled stone when I sign an order for a scan a patient may not need, and I make myself do the old arithmetic first: how much sight, for how much shadow. The stone is still waiting. I would rather not add to it.
- On radiographic contrast as differential X-ray attenuation — dense structures such as bone and metal absorb more of the beam and cast the deeper shadow, and the energy the beam gives up in tissue is deposited as dose — see Jerrold T. Bushberg et al., The Essential Physics of Medical Imaging, 3rd ed. (Philadelphia: Wolters Kluwer / Lippincott Williams & Wilkins, 2012), chaps. 3, 7.↩
- On Leopold Freund's treatment of a five-year-old girl's naevus pigmentosus pilosus beginning 24 November 1896 in Vienna, using apparatus from a photographic institute, and his standing as the founder of radiotherapy, see H. Dietrich Kogelnik, "Inauguration of Radiotherapy as a New Scientific Speciality by Leopold Freund 100 Years Ago," Radiotherapy and Oncology 42, no. 3 (1997): 203-11.↩
- On the second course to the lower back and the resulting X-ray ulcer, which took about six years to heal and left permanent scarring (the patient later traced in good health at seventy-five), see Kogelnik, "Inauguration of Radiotherapy"; Richard F. Mould, "Leopold Freund (1868–1943): Priority for X-ray Therapy," Nowotwory Journal of Oncology.↩
- On Victor Despeignes, the Lyon-trained physician who in July 1896 irradiated a patient's cancer of the stomach at Les Échelles in the Savoie and published the first medical paper on X-ray therapy, and on Emil Grubbé's disputed Chicago claim of January 1896 (for which no contemporaneous documentation survives), see Nicolas Foray, "Victor Despeignes (1866–1937): How a Hygienist Became the First Radiation Oncologist," Cancer/Radiothérapie; Richard F. Mould, "Emil Herman Grubbé (1875–1960) with Special Reference to Priority for X-ray Cancer Therapy," Nowotwory Journal of Oncology.↩
- On the first clearly successful X-ray cures of skin cancer, credited to the Stockholm general practitioners Tage Sjögren and Thor Stenbeck around 1899 (Stenbeck clearing a basal-cell carcinoma over about ninety-nine sessions), see "On the Controversies Surrounding the Origins of Radiation Therapy," Radiotherapy and Oncology 42 (1997); Mould, "Grubbé."↩
- On the early absence of any physical unit and the use of skin erythema (reddening) as the biological gauge of dose, see A Brief History of Radiation Protection Standards (Los Alamos National Laboratory report); K. Sansare, V. Khanna, and F. Karjodkar, "Early Victims of X-rays: A Tribute and Current Perception," Dentomaxillofacial Radiology 40, no. 2 (2011): 123-25.↩
- On the Sabouraud–Noiré pastille of barium platinocyanide (1904), calibrated to change colour with dose and placed on the patient's skin, with "tint B" defined as a full skin-erythema dose against which the epilating dose was gauged, see "Radiation Epilation for Tinea Capitis: A Historical Review," International Journal of Radiation Oncology, Biology, Physics (2012); Otto Glasser, "The Evolution of Dosimeters in Roentgen-Ray Therapy," Radiology 37 (1941): 221.↩
- On the technique of X-ray epilation of the scalp — irradiating in overlapping fields to shed the hair and clear the fungus — see "Radiation Epilation for Tinea Capitis: A Historical Review," IJROBP (2012).↩
- On the scale of childhood scalp irradiation for ringworm — an estimated twenty thousand children treated in the Israeli national campaign between 1948 and 1960, of whom a cohort of some 10,834 was followed for decades — see Elaine Ron et al., "Tumors of the Brain and Nervous System after Radiotherapy in Childhood," New England Journal of Medicine 319 (1988): 1033-39; Siegal Sadetzki et al., "Long-term Follow-up for Brain Tumor Development after Childhood Exposure to Ionizing Radiation for Tinea Capitis," Radiation Research 163 (2005): 424-32.↩
- On the delayed, dose-related excess of meningioma, other CNS tumours, thyroid and head-and-neck skin cancers in the irradiated cohorts (mean brain dose on the order of 1.5 Gy), see Ron et al., "Tumors of the Brain and Nervous System"; Sadetzki et al., "Long-term Follow-up." Treated here as a population-level association, not a claim about any individual.↩
- On the shoe-fitting fluoroscope — its construction, its ten-thousand-plus installations in American shops from the 1920s, and its marketing to children — see Jacalyn Duffin and Charles R. R. Hayter, "Baring the Sole: The Rise and Fall of the Shoe-Fitting Fluoroscope," Isis 91, no. 2 (2000): 260-82.↩
- On foot doses — typically on the order of a tenth of a gray, but reaching close to a gray on the worst machines — with children often scanned repeatedly, see Duffin and Hayter, "Baring the Sole."↩
- On the persistence of the machines despite known harm, the professional warnings of the 1950s, and the bans (Pennsylvania first, in 1957, most states by 1970, effective disappearance by the early 1970s), see Duffin and Hayter, "Baring the Sole"; "History of Radiation Protection," summarising the regulatory sequence.↩
- On Arthur Mutscheller's 1925 proposal of a "tolerance dose," set at roughly one-hundredth of the monthly skin-erythema dose (of the order of a tenth of a roentgen a day, once the unit existed), later taken up by the ICRP, see Arthur Mutscheller, "Physical Standards of Protection against Roentgen-Ray Dangers," American Journal of Roentgenology 13 (1925): 65-70; A Brief History of Radiation Protection Standards (LANL).↩
- On the adoption of the roentgen as the first internationally agreed physical unit of X-ray exposure at the Second International Congress of Radiology, Stockholm, 1928, see A Brief History of Radiation Protection Standards (LANL); "Roentgen (unit)," with the congress proceedings.↩
- On the Monument to the X-ray and Radium Martyrs of All Nations (Ehrenmal der Radiologie), unveiled 4 April 1936 in the garden of St Georg Hospital, Hamburg, under the Deutsche Röntgengesellschaft, bearing 159 names at its unveiling and 359 by 1960, see Werner Molineus, Hans Holthusen, and Hans Meyer, eds., Ehrenbuch der Radiologen aller Nationen, 3rd ed. (Berlin: Blackwell Wissenschaft, 1992); British Institute of Radiology, "1930s Radiology."↩
- Bushberg, Jerrold T., J. Anthony Seibert, Edwin M. Leidholdt, and John M. Boone. The Essential Physics of Medical Imaging. 3rd ed. Philadelphia: Wolters Kluwer, 2012.
- Kogelnik, H. Dietrich. "Inauguration of Radiotherapy as a New Scientific Speciality by Leopold Freund 100 Years Ago." Radiotherapy and Oncology 42, no. 3 (1997): 203-11.
- Mould, Richard F. "Emil Herman Grubbé (1875–1960) with Special Reference to Priority for X-ray Cancer Therapy." Nowotwory Journal of Oncology.
- Foray, Nicolas. "Victor Despeignes (1866–1937): How a Hygienist Became the First Radiation Oncologist." Cancer/Radiothérapie.
- "Radiation Epilation for Tinea Capitis: A Historical Review." International Journal of Radiation Oncology, Biology, Physics, 2012.
- Ron, Elaine, Baruch Modan, John D. Boice Jr., et al. "Tumors of the Brain and Nervous System after Radiotherapy in Childhood." New England Journal of Medicine 319 (1988): 1033-39.
- Sadetzki, Siegal, et al. "Long-term Follow-up for Brain Tumor Development after Childhood Exposure to Ionizing Radiation for Tinea Capitis." Radiation Research 163 (2005): 424-32.
- Duffin, Jacalyn, and Charles R. R. Hayter. "Baring the Sole: The Rise and Fall of the Shoe-Fitting Fluoroscope." Isis 91, no. 2 (2000): 260-82.
- Mutscheller, Arthur. "Physical Standards of Protection against Roentgen-Ray Dangers." American Journal of Roentgenology 13 (1925): 65-70.
- Molineus, Werner, Hans Holthusen, and Hans Meyer, eds. Ehrenbuch der Radiologen aller Nationen. 3rd ed. Berlin: Blackwell Wissenschaft, 1992.