In January 1922, a starving boy in Toronto was given a cloudy extract drawn from an animal's pancreas. The first injection failed. But the second — cleaned up in a biochemist's laboratory — reversed the fatal chemistry of childhood diabetes, and turned what had always been a death sentence back into a life.
A disease measured in bread
Before insulin, childhood diabetes was not really a chronic illness at all — it was only a postponement. A child would come in thirsty and thin, with a faint sweetness on the breath, wasting away in a manner that no amount of food could repair. The urine ran heavy with sugar because the blood was heavy with it, and the body, unable to use the fuel it carried, slowly began to consume itself. Fat burned down into acids, the breathing grew deeper, and the mind began to cloud. At the end there was coma, and after the coma there was simply no child.1
The best a physician could do was to slow the dying by starvation. Frederick Allen's severe diet had become the hard mercy of the pre-insulin years: bread and calories were counted down and down, until the body was left with almost nothing from which sugar might rise. In a strong adult it bought time. In a child it often bought no more than a thinner death. The photographs that survive from those wards do not look like ordinary illness; they look like famine, conducted under medical supervision.2
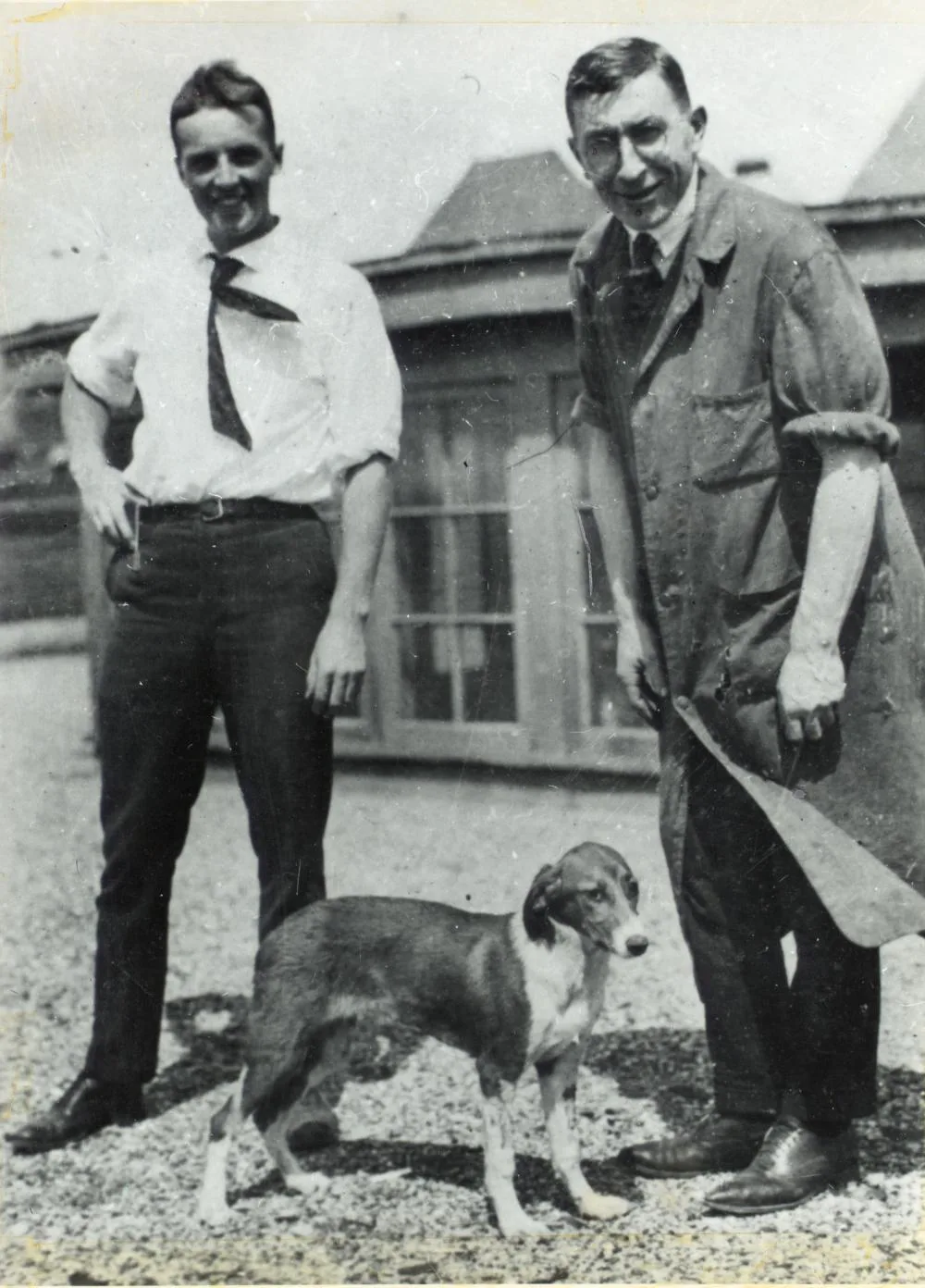
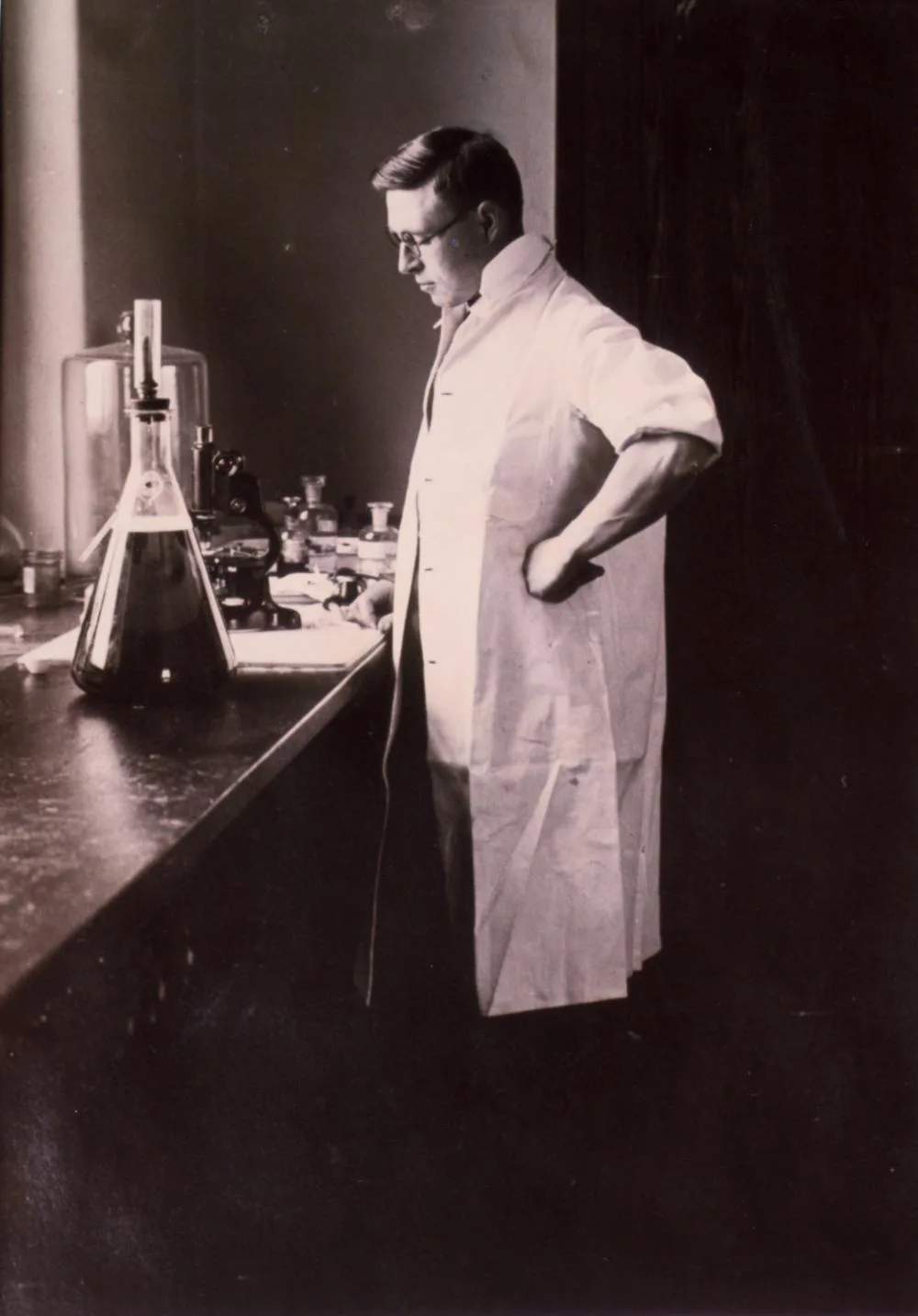
This was the disease that Frederick Banting believed he might be able to reach. He was no great physiologist when the thought first came to him — only a young Canadian surgeon, recently back from war service, restless in a small practice and teaching a little on the side at Western University. Late in 1920, after reading about the pancreas and its degenerated ducts, he scribbled down the rough idea that would one day carry him to Toronto: tie off the pancreatic ducts, wait for the digestive acini to degenerate, and then try to recover the organ's internal secretion from the islet-rich remnant left behind.3 It was hardly a polished theory. It was a surgeon's gambit, thrown at what was really a biochemical problem.
J. J. R. Macleod, the professor in Toronto, gave him a little space, some dogs, and a student assistant. The student was Charles Best. The work began in May 1921, in the old medical building — not as a clean miracle, but as a long summer of clumsy operations, infected wounds, failed ligatures, and dead animals. And yet some of the animals did respond. When pancreatic extract was injected into pancreatectomised dogs, the sugar in their blood could be made to fall. Dog 410 appeared to show the effect and then died the next day; others, among them 406 and 408, responded just enough to keep the claim alive — while showing, at the same time, how fragile the whole enterprise still was.4
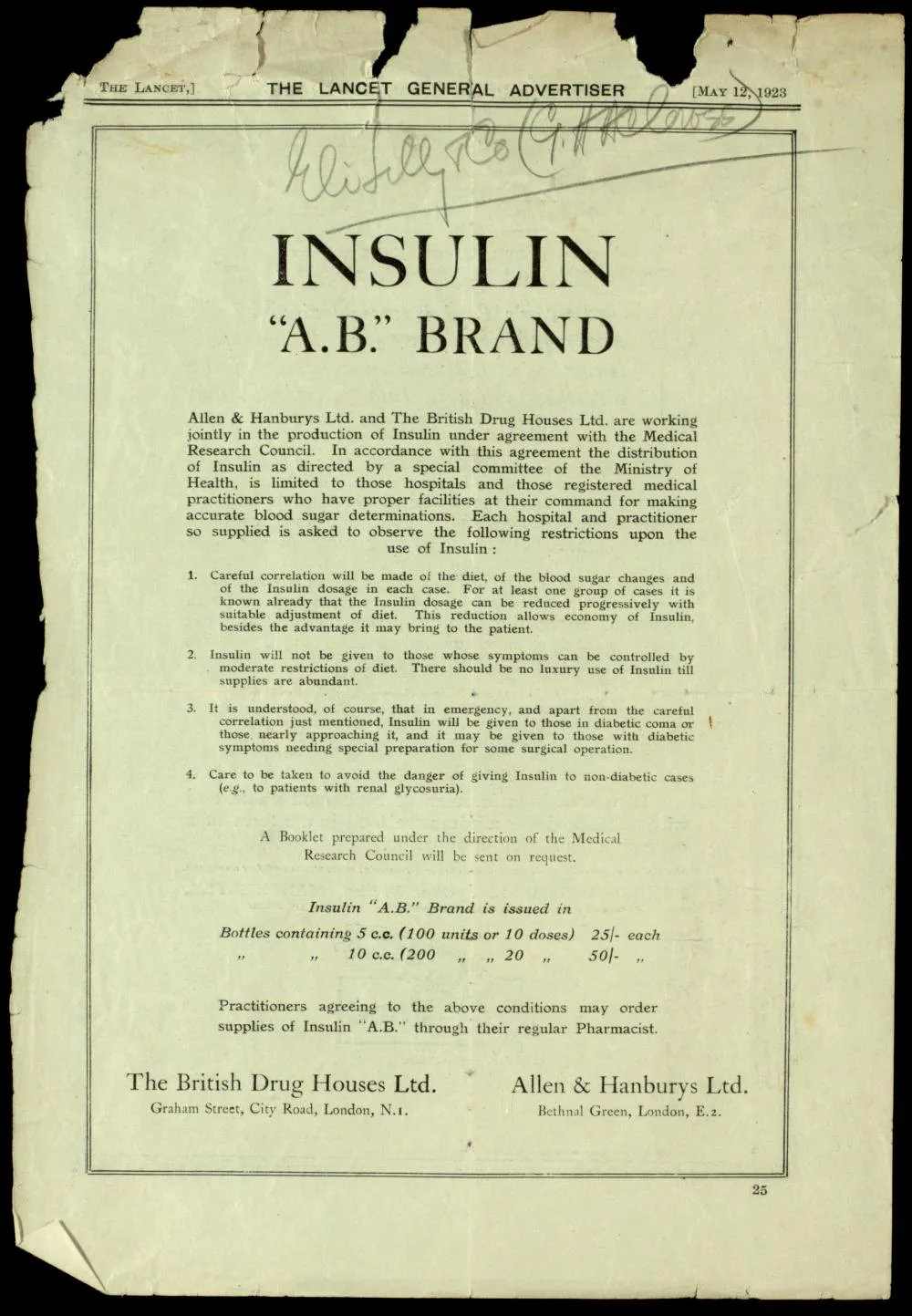
The extract itself was still crude — brown, irritating, unstable, and made in quantities far too small for the disease that was waiting outside the laboratory door. Banting and Best widened the sources and the scale of their pancreas work, yet the material remained difficult to test and harder still to reproduce. When Macleod returned from Europe, he pushed the work into more orderly shape, and late in 1921 James Bertram Collip, a biochemist from Alberta, joined the effort and set about doing the one thing the surgeons could not: purifying it.
Leonard Thompson
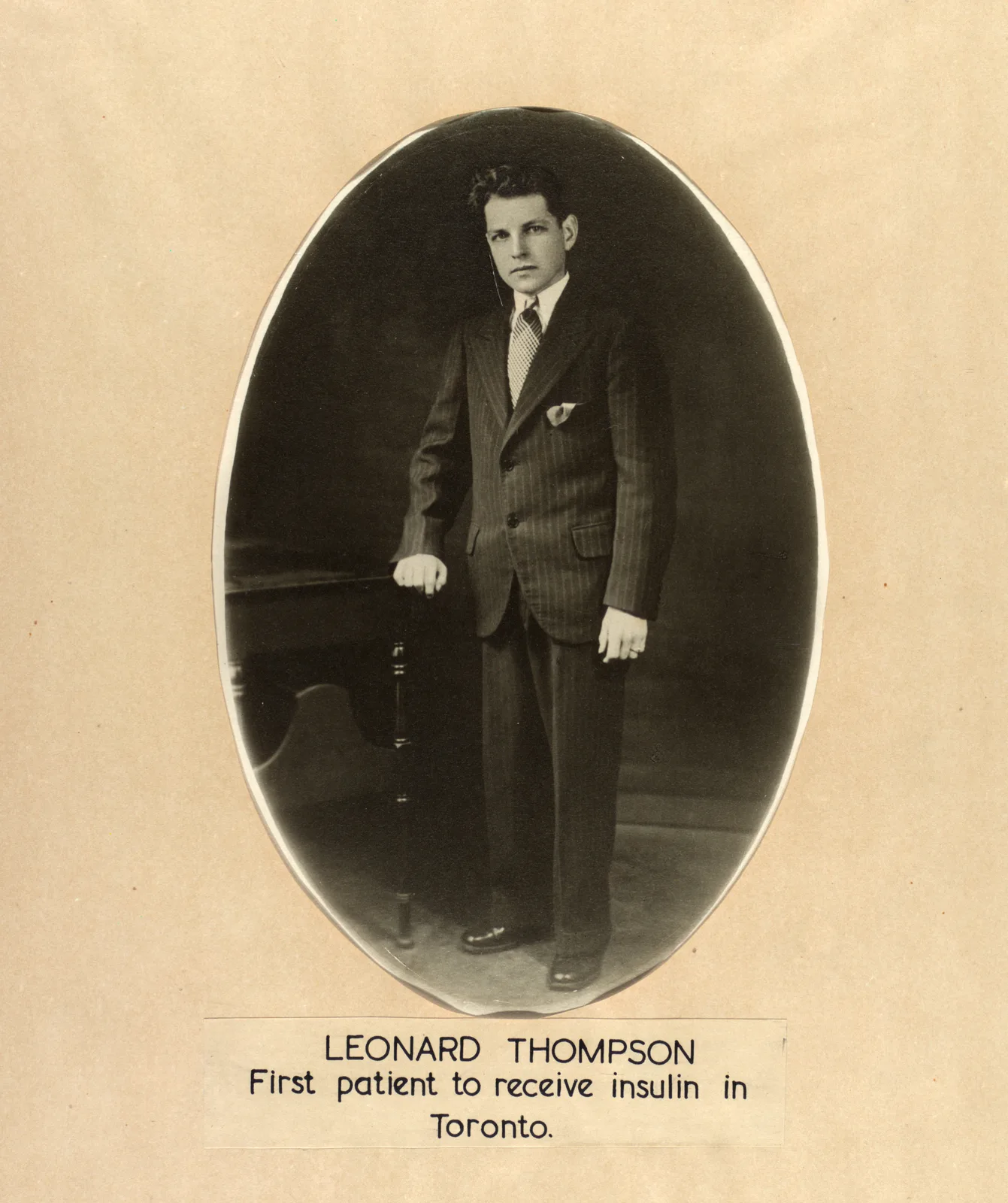
The first patient to be injected was not a whole row of children waking one by one; that picture belongs to the fonder, later image insulin would soon earn. The patient was a single boy. Leonard Thompson was a charity case on a public ward at Toronto General Hospital, a teenager whom diabetes had already reduced to starvation weight, kept barely alive by diet and very nearly spent. On 11 January 1922 he received Banting and Best's extract — and the injection was not the resurrection the later story would want it to be. It caused a sterile abscess and did little in clinical terms. His blood sugar fell only modestly, the ketones stayed where they were, and by the standards the team had been hoping for, the attempt was a failure.5
Twelve days later they tried again, this time with Collip's cleaner extract, and now the change was exactly the one the first injection had promised but failed to deliver. Leonard's blood sugar fell sharply. The sugar all but disappeared from his urine, and the ketones vanished from it entirely. His condition improved in a way that no starvation diet could possibly explain.6 What matters about that moment is its double nature: insulin did not arrive as a single, pure discovery, but as a rescue that had to pass through failure, purification, and a second needle before it could become medicine.
Even the name was still unsettled. Banting and Best had written "isletin" in a few notebook entries; it was Macleod who would soon propose "insulin", after the islets of Langerhans, and it was his word that endured. The question of ownership was unsettled too, and it would stay poisonous for years. Banting was certain that the idea and the labour had been his and Best's. Macleod believed, not without reason, that the work had needed a physiologist's laboratory and a physiologist's standards before it could stand at all. And Collip, in the narrowest but most decisive sense of all, was the one who had made the extract fit for a human being. When the Nobel Prize came in 1923, awarded to Banting and Macleod, it cut the quarrel into an official shape without ever quite settling it; Banting shared his prize money with Best, and Macleod shared his with Collip.7
But the boy in the public ward had far less stake in the question of priority than in a far simpler fact: death had begun to loosen its grip on him. After Leonard, the trials widened, and other Toronto patients began to improve as well. Theodore Ryder, treated in the summer of 1922 as a wasting child, would later write back with the blunt, happy triumph of a boy restored to his appetite and his flesh. Elizabeth Hughes, daughter of the American statesman Charles Evans Hughes, arrived skeletal after years of Allen's diet and recovered so far that she became, first in private and then in the public record, one of insulin's most durable witnesses. Elsie Needham, found comatose at the Hospital for Sick Children in October 1922, became the first child recorded in Toronto to recover from a diabetic coma after treatment.8
It is here that the legend very nearly becomes true — though never all at once, never down a single theatrical row of beds, and never without its own deaths and shortages and bouts of frantic manufacturing. Yet in ward after ward the old sequence did begin to fail. The child no longer had to pass inevitably from thirst to wasting to acidotic stupor to death. Sometimes the breathing settled. Sometimes the urine cleared. Sometimes the patient woke.
Read from the Ward
On the nights when diabetic ketoacidosis comes through the unit, the first clue is often the breathing — deep, fast, almost mechanical, a body labouring to blow off acid. We hang fluids, replace potassium, and hunt for the infection or the infarction that tipped the patient over the edge; but underneath all of that urgent work lies a single, simpler absence. And that is exactly what makes Leonard Thompson's second injection so startling even now. Once insulin is restored, the body's whole accounting changes: sugar can move into the cells again, and the acidotic spiral slowly begins to unwind. The patient who seemed to be drowning in his own chemistry comes back — not because we have fought each symptom one by one, but because we have given back the single signal around which the entire disorder was organised.
This is why the Toronto work feels so unlike an ordinary drug discovery. Penicillin kills an invader; ether silences consciousness. Insulin is a stranger thing than either. It is a message the body was always meant to send to itself, handed back to it from the outside. In type 1 diabetes the treatment is not a foreign weapon at all, but a missing grammar — a way of telling the liver, the fat, and the muscle that there is plenty to go around, and that the body can stop devouring itself.
By our standards the early extract was filthy, and the dosing was little more than educated guesswork. No one in that ward had a glucometer, a potassium protocol, an infusion pump, or any modern sense of cerebral oedema. What they had to go on was urine, breath, appetite, weight, and survival. And yet they had crossed the one boundary that truly mattered. A disease that had once been measured out in bread could now be measured in units.
There is a real temptation, in telling this story, to make Banting the lone hero and the boy merely the proof of him. The truer reading is less tidy, and far more useful. Banting supplied the obsession, Best the hands, Macleod the laboratory and the standard of proof, Collip the purification, and Leonard Thompson the terrible human test. The miracle never belonged to any one man; it belonged to a chain of people, each of whom held one necessary piece of it.
Leonard did not go on to live a normal life, at least not by modern standards. He survived thirteen more years and died in 1935, still young, of broncho-pneumonia and complications from his diabetes.9 But those thirteen years were not a footnote. For a child who had been carried into Toronto General in what should have been the last winter of a fatal disease, they amounted to an era. Insulin did not abolish diabetes; what it did was change its grammar — from a sentence into a condition, from a countdown into an argument that patient and physician could go on having with the body, year after year.
That is the quiet grandeur of the public ward. The boy was not cured. He was given back to time.
- University of Toronto Libraries, "The Terrors of Diabetes," Insulin 100, on pre-insulin diabetes as a frequently fatal wasting disease, especially in children.↩
- University of Toronto Libraries, "Patients," Insulin 100, describes the pre-insulin condition of children treated with starvation diets and the transformation after insulin.↩
- University of Toronto Libraries, "Banting's Idea," Insulin 100; see also Michael Bliss, The Discovery of Insulin, 25th anniversary ed. (Chicago: University of Chicago Press, 2007).↩
- University of Toronto Libraries, "The Summer of 1921," and "Growing the Team," Insulin 100.↩
- University of Toronto Libraries, "First Clinical Trials," Insulin 100; F. G. Banting, C. H. Best, J. B. Collip, W. R. Campbell, and A. A. Fletcher, "Pancreatic Extracts in the Treatment of Diabetes Mellitus," Canadian Medical Association Journal 12 (1922): 141-46.↩
- Banting et al., "Pancreatic Extracts," 143-45; University of Toronto Libraries, "First Clinical Trials."↩
- Nobel Prize Outreach, "The Nobel Prize in Physiology or Medicine 1923"; University of Toronto Libraries, "The Struggle for Glory," Insulin 100.↩
- University of Toronto Libraries, "Resurrections in Toronto," and "Patients," Insulin 100.↩
- University of Toronto Libraries, "Patients," Insulin 100, notes Leonard Thompson's later life and death in 1935.↩
- Banting, F. G., C. H. Best, J. B. Collip, W. R. Campbell, and A. A. Fletcher. "Pancreatic Extracts in the Treatment of Diabetes Mellitus." Canadian Medical Association Journal 12 (1922): 141-46.
- Bliss, Michael. The Discovery of Insulin. 25th anniversary ed. Chicago: University of Chicago Press, 2007.
- Nobel Prize Outreach. "The Nobel Prize in Physiology or Medicine 1923." NobelPrize.org.
- University of Toronto Libraries. Insulin 100: Discovering Its History. Fisher Digitus, 2021.