In the operating theatres before 1846 the greatest surgeon was the fastest one. Robert Liston could have a leg off in under half a minute, and he was celebrated for it, because his patient was awake and held down and every second under the knife was borne in full. Then ether stopped the clock. Surgery could at last be slow, deliberate, and deep. What no one saw was that the screaming had been doing a kind of work, and that silencing it a full generation before anyone understood infection would open the interior of the body to a new and quieter way of dying.
The virtue of speed
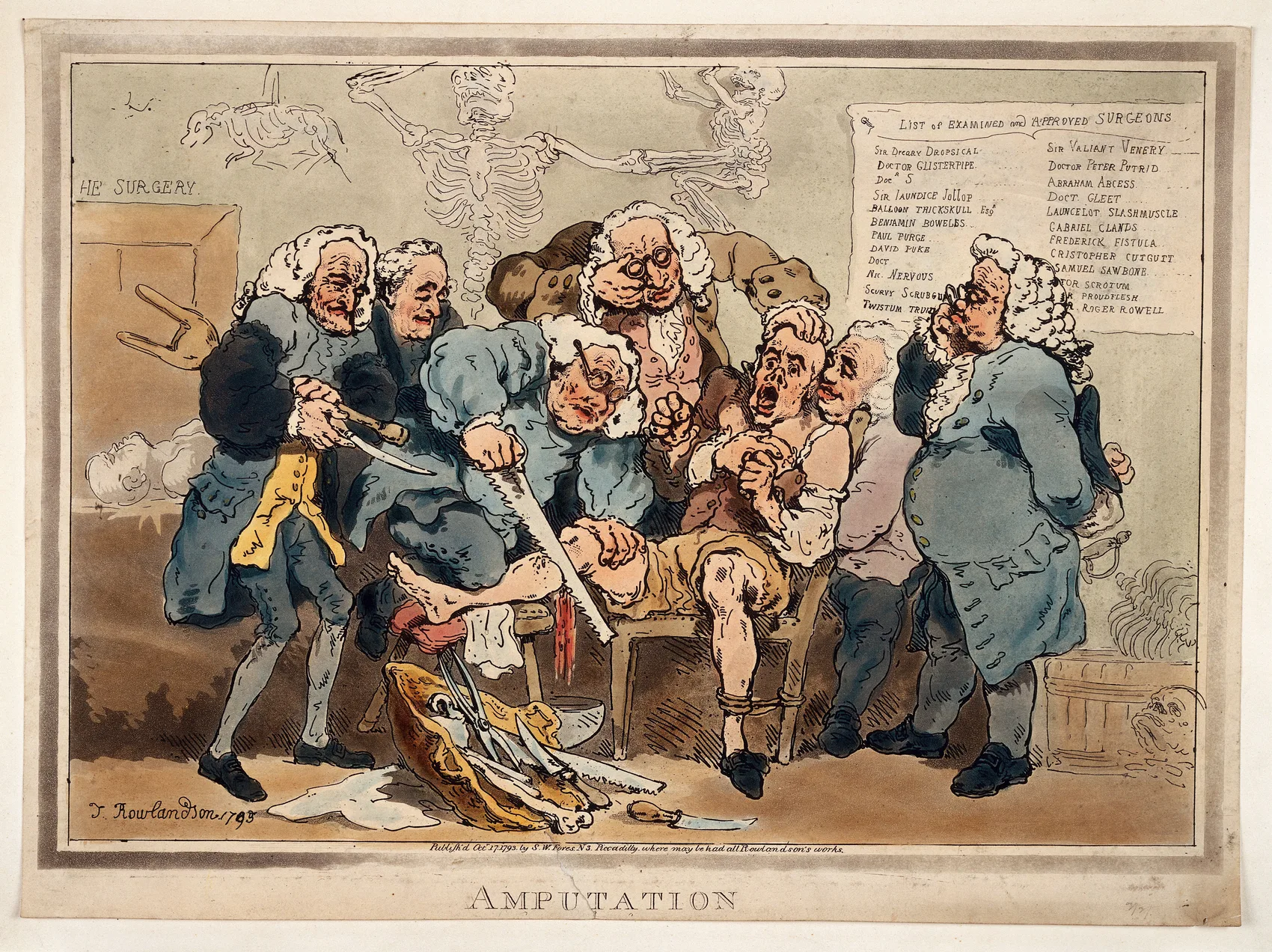
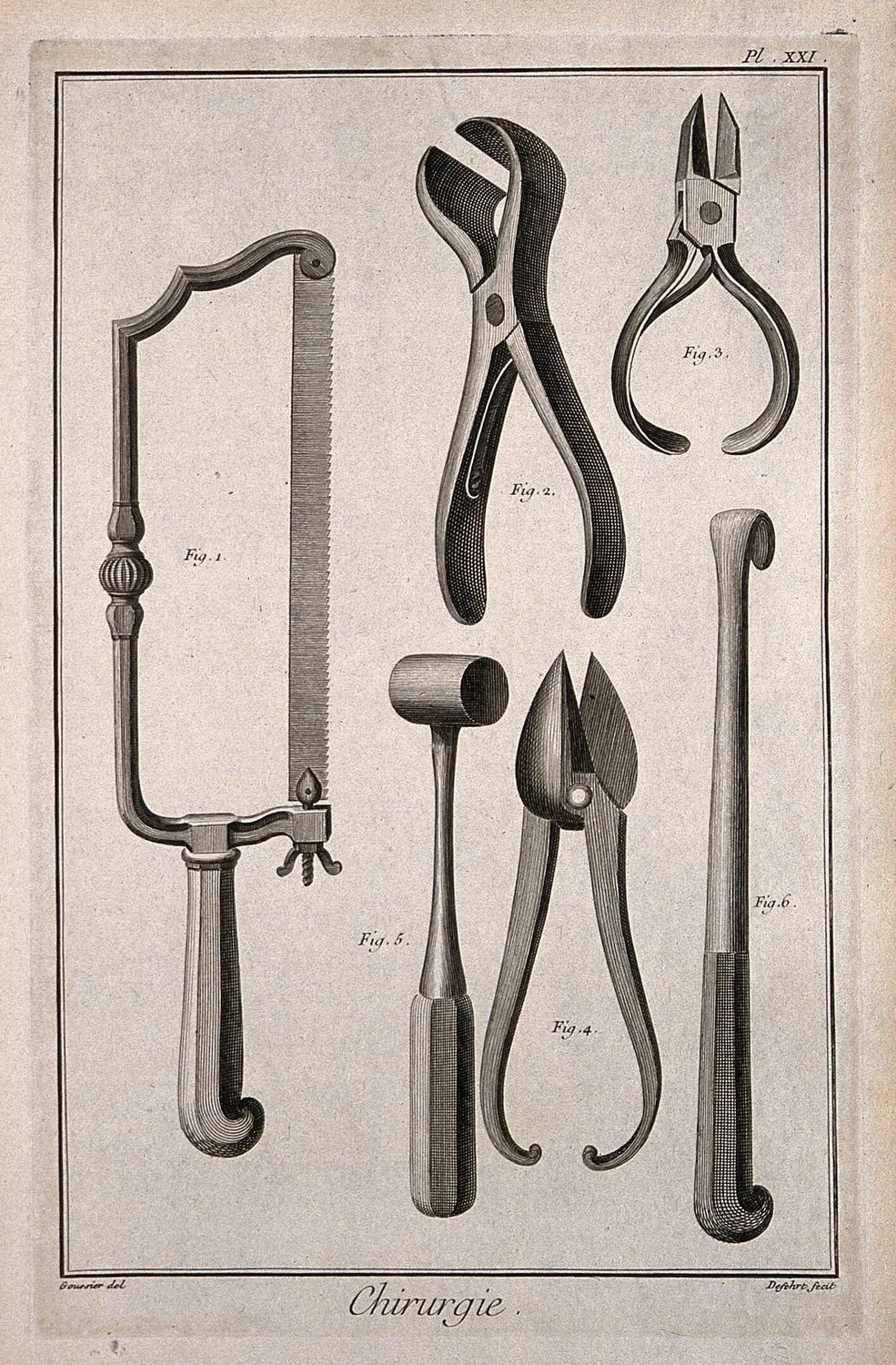
For as long as surgery had existed, its supreme skill was speed. A patient on the table was conscious, pinned by assistants, and enduring pain of a kind that the modern world has almost no memory of; the only mercy the surgeon could offer was to be quick.1 The great operators of the age were timed the way athletes are timed. Robert Liston, the towering Scot who dominated the London theatres, was known as the fastest knife in the West End, able at his fastest to have a limb off in around half a minute, the leg gone and the vessels tied before a slower man had well begun.2 Students packed the galleries to watch him work against the clock.
Speed was never vanity; it was the whole strategy of an impossible craft, and it set the limits of what surgery could attempt. An operation had to be finished in the time a human being could endure being cut, which meant the surface of the body and the limbs, the quick amputation and the rapid excision. The chest and the abdomen, where no operation could be done in a minute, were very largely forbidden country. The awake, suffering patient was a clock that governed everything, and the clock would not give more than a few minutes.
The clock stops
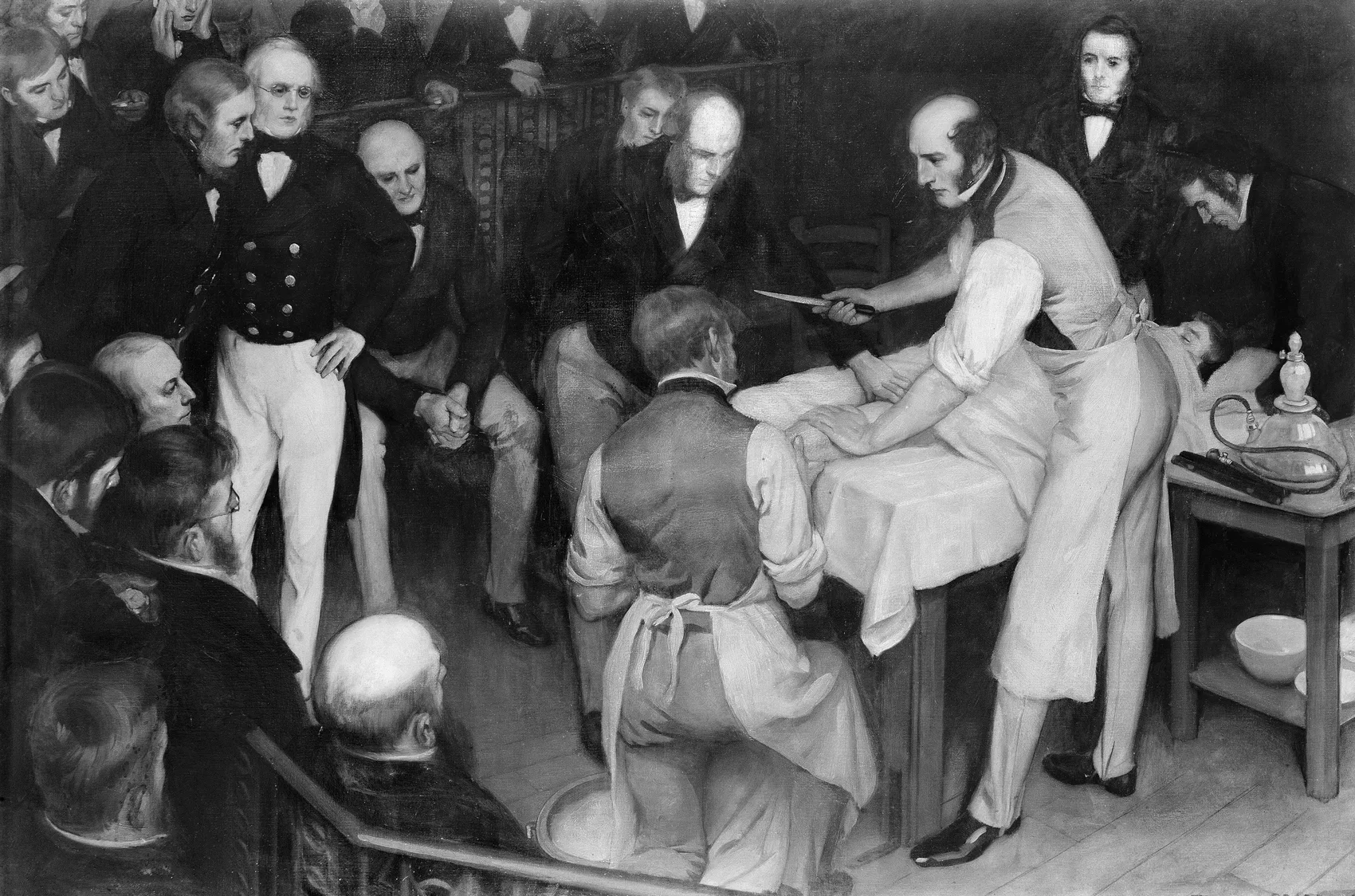
The man who best embodied surgical speed was also the man who announced the end of its reign. On the twenty-first of December 1846, just over nine weeks after ether was first shown in Boston, Robert Liston used it at University College Hospital in London to amputate the diseased leg of a butler named Frederick Churchill, in what is remembered as the first operation under anaesthesia in Europe.3 The leg came off in well under a minute, as fast as it ever had; the difference was that Churchill felt none of it, and woke to ask when the surgery was going to begin. Liston, not a sentimental man, turned to the gallery and said, "This Yankee dodge beats mesmerism hollow."4
He had spent his life proving that a surgeon's worth was measured in seconds, and in a single morning he showed that it need not be. With the patient asleep, the clock that had governed surgery since antiquity simply stopped. There was no longer any reason to hurry. An operation could be slow, careful, and exact; it could pause to consider; it could go where speed had never let it go, into the abdomen and the chest and, in time, the skull.5 The abolition of pain did not merely spare suffering. It removed the single hardest constraint the craft had ever worked under, and the surgeons of the day understood at once that the map of what was possible had been torn up.
The unbraking
Here the story is usually allowed to end, in triumph. It should not, because the constraint that ether removed had been doing more than one job. Pain had made surgery brief, and brevity, it turned out, had been holding back a catastrophe that no one yet understood.
Freed of the clock, surgeons operated more, and longer, and deeper. They opened cavities they had never dared to open, and they did it in the same crowded, unwashed wards, with the same unclean hands and instruments, that had always been there, because this was still twenty years before the germ was understood and the wound was thought to suppurate by its own nature.6 The result was that patients who would once have been spared the knife now survived the operation and died of the wound. The great killers were the so-called hospital diseases, and they had a collective name: James Young Simpson called it hospitalism, the pyaemia and erysipelas and hospital gangrene that swept the surgical wards and turned a clean amputation into a lethal infection days later.7 Mortality after amputation in the great hospitals ran appalling: around two in three after a thigh amputation in the Paris hospitals of the mid-century, and higher still in some wards.8
Anaesthesia, taken by itself, did not lower the death rate of surgery, and in some wards it arguably raised it, because it invited more surgery and deeper surgery into an environment that could not yet keep a wound clean. The gift of painlessness had arrived a full generation before the knowledge that would make it safe to use, and the interval between the two was paid for in lives.
The two halves of a gift
The second half of the gift came in 1867, when Joseph Lister, building on Pasteur, argued that the wound rotted because living organisms entered it, and that they could be kept out.9 Only when the abolition of pain was joined to the exclusion of infection did surgery become the thing we now recognise, a reasonable bet rather than a desperate one. Lister's own figures made the point with brutal clarity: in the years before he adopted antiseptic method his mortality in major operations ran near forty-six in the hundred, and in the years after it fell to about fifteen.10
For twenty-one years the world had the first half without the second. It could put a patient to sleep and take its time, and it used that freedom to reach further into the body than ever before, and for two decades the reaching killed more than it saved. The lesson buried in that interval is not that anaesthesia was a mistake, but that a new power in medicine almost always arrives before the discipline that makes it safe, and that the gap between the two is the most dangerous place a patient can stand.
Read from the Ward
Before every operation in my hospital there is a pause. The room stops; a nurse reads the patient's name aloud, the procedure, the side to be cut, the allergies, the count of instruments that must all be accounted for again at the end. It takes under a minute, and it is enforced with a seriousness that surprises people who imagine an operating theatre as a place of pure momentum. We call it the time-out, and it is, precisely, a brake: a small deliberate delay engineered into a process that spent a century learning to be fast.
I think about Liston's clock when I stand through one of those pauses. His century prized speed because a screaming patient demanded it, and then anaesthesia took the scream away and let surgery slow down, and the slowing down was a genuine good that also, for a generation, let surgeons hurt people in new ways because nothing was holding them back. What strikes me is not that they were reckless. It is that the restraint they lost had never been chosen; it had been imposed on them by pain, and when pain lifted, the restraint lifted with it, and no one noticed the brake was gone until the wards filled.
That is the pattern I actually watch for now, and it has almost nothing to do with surgery in particular. Every real advance I have seen arrives the same way. A drug that works arrives before we understand what it does at the edges. A monitor that lets us intervene arrives before we have learned when not to. A technique that lets us reach a place in the body arrives before we know what it costs to go there. The capability comes first, clean and exciting, and the wisdom to bound it comes later and slower, assembled out of the harm done in between. The interval is never skipped. It can only be shortened, by people who are looking for it.
So the pause is not really about the checklist. It is medicine putting back, on purpose and with full knowledge, a brake that a great gift once removed by accident. We spent the first century after ether learning that the abolition of a constraint is not the same as the mastery of what the constraint was holding back. The awake patient's clock is gone, and I am glad it is gone. But I have come to respect what it was quietly doing, and a good part of what my colleagues and I build into every procedure now is an attempt, in cooler and more deliberate form, to keep doing it.
- On speed as the paramount virtue of pre-anaesthetic surgery, dictated by the conscious, unanaesthetised patient, see Harold Ellis, A History of Surgery (London: Greenwich Medical Media, 2001); Richard Hollingham, Blood and Guts: A History of Surgery (London: BBC Books, 2008).↩
- On Robert Liston as "the fastest knife in the West End," whose fastest amputations were timed in seconds (his quickest at around half a minute, though his routine operating times ran longer), see "Robert Liston," Royal College of Surgeons of England, Plarr's Lives of the Fellows; Ellis, A History of Surgery.↩
- On Liston's amputation of the leg of Frederick Churchill under ether at University College Hospital on 21 December 1846 — the first operation under anaesthesia in Europe — see Ellis, A History of Surgery; "The History of Anaesthesia," World Federation of Societies of Anaesthesiologists.↩
- The remark "This Yankee dodge beats mesmerism hollow," attributed to Liston after the ether amputation, is widely reported; the patient Churchill is said to have asked when the operation would begin. See University College London historical accounts; Ellis, A History of Surgery. Treated here as well-attested tradition.↩
- On anaesthesia opening previously "forbidden" areas — the abdomen, chest and, later, the cranium — to deliberate, unhurried surgery, see "The History of Anaesthesia," WFSA; "The New World of Surgery," in Emotions and Surgery in Britain, 1793–1912 (Cambridge University Press).↩
- On the persistence of unclean wards, hands and instruments in the two decades before germ theory and antisepsis, and the belief that wounds suppurated by their own nature, see W. F. Bynum, Science and the Practice of Medicine in the Nineteenth Century (Cambridge University Press, 1994).↩
- On James Young Simpson's coinage of "hospitalism" for the pyaemia, septicaemia, erysipelas and hospital gangrene of the surgical wards, see James Y. Simpson, "Hospitalism: Its Effects on the Results of Surgical Operations," Edinburgh Medical Journal (1869); and A. G. McKenzie, "The Bicentenary of James Young Simpson," Anaesthesia 66 (2011).↩
- On amputation mortality of roughly two-thirds in the mid-century Paris hospitals, see "The History of Anaesthesia," WFSA; on comparable British figures, see the amputation-mortality literature of the 1850s (e.g. the London Hospital returns).↩
- Joseph Lister, "On the Antiseptic Principle in the Practice of Surgery," The Lancet (1867); Lister's system is treated in this Codex under On the Antiseptic Principle (Plate XXIII) and The Carbolic Spray (Plate XXIV).↩
- On the fall in Lister's own operative mortality from about 45.7 per cent (1864–66, before antiseptic method) to about 15 per cent (1867–69, after), see the Lister mortality data discussed in "Hand in Hand — Anaesthesia and Antisepsis," ESAIC; the James Lind Library on the antisepsis controversy.↩
- Ellis, Harold. A History of Surgery. London: Greenwich Medical Media, 2001.
- Hollingham, Richard. Blood and Guts: A History of Surgery. London: BBC Books, 2008.
- Bynum, W. F. Science and the Practice of Medicine in the Nineteenth Century. Cambridge: Cambridge University Press, 1994.
- McKenzie, A. G. "The Bicentenary of James Young Simpson (1811–1870)." Anaesthesia 66 (2011): 1149-54.
- Simpson, James Y. "Hospitalism: Its Effects on the Results of Surgical Operations." Edinburgh Medical Journal (1869).
- Lister, Joseph. "On the Antiseptic Principle in the Practice of Surgery." The Lancet 90 (1867): 353-56.
- "The History of Anaesthesia." World Federation of Societies of Anaesthesiologists.
- "Hand in Hand — Anaesthesia and Antisepsis: A Historical Perspective." European Society of Anaesthesiology and Intensive Care (ESAIC).
- "Robert Liston." Royal College of Surgeons of England, Plarr's Lives of the Fellows.